GreyMatters
Educational articles, BetterBrain resources, latest in brain health, and news about us. Written for you, with expertise (and love).
VERVE-102: A One-Time Gene Edit for Cholesterol, and Why It's a Brain Story | BetterBrain
Every so often a piece of research comes along that makes you stop and appreciate how far medicine has come. This is one of those.
Researchers just reported early results for a one-time treatment that durably lowers LDL cholesterol by editing a single gene. One infusion, with effects that have held for up to a year and a half so far, and likely to last a lifetime. It's very early research in a small, specific group of patients, and it's years from a doctor's office. But the underlying biology is some of the most well-studied in all of cardiovascular medicine, and it connects directly to your brain.
Editing one gene to lower cholesterol
The therapy, called VERVE-102, targets a gene called PCSK9. PCSK9 is a protein that reduces your liver's ability to clear LDL cholesterol from your blood. The more PCSK9 activity you have, the fewer LDL "receptors" your liver keeps available to pull LDL particles out of circulation.
Here's the reassuring part: some people are born with naturally low-functioning PCSK9 genes, and they tend to have markedly lower LDL across their entire lives, substantially lower rates of heart disease, and no apparent downside. Turning down PCSK9 is a protective pattern scientists have studied for two decades. We already have approved PCSK9-lowering drugs; they just require ongoing injections.
What's new is the delivery. VERVE-102 uses base editing, a precise form of gene editing, to make a single change to the PCSK9 gene in liver cells after one infusion, doing once, durably, what current drugs do repeatedly. In the Heart-2 trial, a single dose lowered LDL by an average of around 50%, and by as much as roughly 69% at the higher doses, with reductions holding for up to 18 months and no treatment-related serious adverse events reported.
The honest caveats
The headline is easy to over-read, so here's the careful version. It's a phase 1b trial, an early stage focused on safety and initial signals in a small number of participants, and it has not been shown to prevent heart attacks, strokes, or cognitive decline. It enrolled a specific, high-risk group (inherited very high cholesterol or early coronary artery disease), so these are not general-population results. And gene editing is genuinely new: the PCSK9 mechanism is exceptionally well understood, but a permanent edit to a gene is a young field whose long-term safety story takes years to write. The likely path is approval first for very high-risk individuals, at significant cost, after a larger phase 2 trial.
Why this is a brain-health story
At BetterBrain, we look at the whole body, because your brain doesn't exist in isolation from it, and few things connect the two as directly as lipids.
Start with ApoB. You've probably heard of LDL cholesterol; ApoB is the more precise number underneath it. Every LDL particle carries exactly one ApoB protein, so LDL-C tells you the amount of cholesterol in LDL particles, while ApoB tells you the number of particles actually driving damage in your artery walls. When the two disagree, ApoB is the better predictor of risk. Lowering PCSK9, through these new therapies or the drugs we already have, lowers both.
Now connect it to the brain. The blood vessels that feed your brain face the same lipid-driven damage as the ones feeding your heart, and that vascular damage is one of the major pathways of cognitive decline. Protecting your lipids over a lifetime is protecting your brain, especially for people who tend to run higher LDL, including APOE4 carriers. That's one reason lipid management is a core part of what we do.
What this means for you, right now
You don't have to wait for a therapy that's years away. The target itself, your lipid health, is something you can measure and move today.
Get your ApoB tested, not just standard cholesterol, because it counts the particles actually driving damage. Think of lipids as a lifelong number: it's the decades of cumulative exposure that drive risk, so small, steady improvements compound in your favor, and starting earlier beats starting perfectly. Use the levers you already have, including diet, regular movement, and, where your physician recommends them, proven medications.
If you'd like to see where you stand, BetterBrain Blueprint covers ApoB and 50+ other markers and starts at $89 with insurance, and a BetterBrain coach can pull your full lipid picture into one clear plan, so that whatever arrives in five or ten years, you've protected the decades in between.

The Glymphatic System: Why Deep Sleep Is Your Brain's Best Cleanup Tool
What if the most important thing you could do for your brain tonight was also the most straightforward? Not a new supplement or a complicated protocol. Just better sleep, specifically the deep stages most people shortchange without knowing it.
Here is the biology that makes that matter more than most people appreciate.
Your brain has its own plumbing. It only fully runs at night.
Every other tissue in your body has a lymphatic system to carry away metabolic waste. For a long time, the brain was thought to be the exception, with no obvious mechanism for the job. That changed in 2013 when researchers described the glymphatic system: a network that uses cerebrospinal fluid to flush waste out of brain tissue, including amyloid-beta and tau, the proteins that accumulate in Alzheimer's disease.
The connection to sleep came alongside it. Glymphatic clearance is not constant. It ramps up dramatically during deep, slow-wave sleep, when the spaces between brain cells expand and fluid can move through more freely. This is one of the clearest biological explanations for why sleep is not optional maintenance. It is when a specific, measurable cleanup process actually runs, protecting your brain now and building resilience for decades to come.
What the newer research tells us about the engine
The system's existence has been well established for over a decade. What researchers kept working on was the mechanics: what physically moves the fluid?
A 2025 study published in Cell from Maiken Nedergaard's lab (one of the teams behind the original glymphatic work) helps answer that. In mice, the team found that during deep sleep a small brainstem region called the locus coeruleus releases norepinephrine in slow, rhythmic waves, roughly one every fifty seconds. Each wave gently tightens and relaxes the blood vessels, and that slow oscillation appears to drive cerebrospinal fluid through the brain, moving waste along.
The result connects three things already known to be related (deep sleep, blood-vessel tone, and fluid clearance) into a single mechanism. Deep sleep is not the brain idling. It is the brain running a coordinated pump.
Two points of context worth holding on to. First, this is animal research. The mechanism has been demonstrated in mice, whose sleep biology is a strong but imperfect model for humans. It tells us how the system likely works, not the conclusion of a human clinical trial.
Second, the same study found that zolpidem (the active ingredient in Ambien) suppressed these norepinephrine waves in mice and reduced fluid flow. That is a genuinely interesting signal, but it is a finding in animals about a mechanism, not evidence that a prescription harms people. If you take a sleep aid, this is not a reason to stop. It is a reason to make sleep quality a real conversation with your prescriber.
What this means in practice
None of this requires a new gadget. It gives you a sharper reason to take the fundamentals seriously.
Protect the deep-sleep window. Slow-wave sleep is concentrated in the first half of the night. A consistent wake time, morning light exposure within thirty minutes of getting up, and a cool, dark room are the most reliable ways to support it. These are habits that compound over years.
Be honest about alcohol and late meals. Both fragment the deep-sleep stages where clearance is most active. You may fall asleep quickly and still miss the part of the night that matters most for this system.
Treat sleep as something measurable. The same way we use biomarkers to track what is working, sleep consistency and quality are worth paying attention to over time rather than estimating from how you feel in the morning.
Take loud snoring or daytime exhaustion seriously. Both can signal sleep apnea, which repeatedly disrupts the deep sleep this system depends on. It is common, often undiagnosed, and very treatable.
If you use a sleep medication, bring the goal of better sleep quality to your prescriber rather than changing anything on your own.
BetterBrain's brain health coaches work with clients to turn sleep from a vague intention into a specific, trackable practice built around your schedule, your biology, and your data. Think sharper now, and protect your brain for decades.

Tommy Wood's 3-S Model: The Science Behind Future-Proofing Your Brain
The Framework Behind What We Do at BetterBrain
Our Chief Science Officer Tommy Wood published The Stimulated Mind in March 2026, and we think it's the most complete, accessible guide to dementia prevention that exists right now. A rigorous, science-backed model for understanding what your brain actually needs across a lifetime, written by someone who has spent his career studying exactly this.
At the center of the book is what Tommy calls the 3-S Model: Stimulation, Support (sleep and recovery), and Supply (of energy and nutrients). These aren't three separate suggestions. They're three categories of input the brain depends on, and Tommy's argument is that they reinforce each other in ways most people don't appreciate. They synergize, providing outsized benefits from even simple changes across all three.
BetterBrain is built around exactly this model. The 10 health systems and 11 practices our coaches work through with you are the operational version of what Tommy lays out in the book. Here's a breakdown of each S and one thing you can act on this week.
S1: Stimulation
The first S is the one that surprises people. Tommy's argument is that the brain, like muscle, needs ongoing challenges to maintain its structure. The variable that matters is novelty. Doing the same crossword every day is not stimulation in the sense your brain cares about. Learning a language, picking up a new instrument, or taking a class on something you have no prior context for, are stimulating.
This connects to what researchers call cognitive reserve: the buffer your brain builds through years of varied learning. Cognitive reserve is one of the strongest predictors of who maintains function in their 70s and 80s, even in the presence of pathology like amyloid plaques.
What you can do this week: Pick one thing this month that you don't already know how to do. It doesn't have to be heavy, a new recipe technique, a new fitness class, a new route on your morning walk that requires you to navigate. The brain treats novelty as a signal that it needs to keep adapting.
S2: Support (Sleep and Recovery)
The second S is the one most people know is important and still underestimate. Recovery, especially during sleep, is when the brain adapts and improves.
While you sleep, your brain runs a waste-clearance system that flushes out the proteins that build up during the day, including amyloid, the same protein that accumulates in Alzheimer's disease. Think of it like a dishwasher that only runs at night. Skip enough nights, or get consistently shallow sleep, and the dishes pile up. Disrupted sleep is associated with elevated pTau-217, lower cognitive scores, and higher long-term dementia risk.
Tommy is direct about this in the book: there is no supplement protocol that compensates for chronically poor sleep. And the work has to start with the structure of your sleep itself, meaning how much time you actually spend in the deep and REM stages, not just how many hours you're in bed. You can sleep eight hours and still miss most of the stages where the real restoration happens.
What you can do this week: Protect a consistent wake time. The wake time matters more than the bedtime because it anchors your body's internal clock. Pair it with morning light within 30 minutes of getting up, and you've done more for your sleep quality than most people manage with supplements or sleep trackers alone.
S3: Supply (Energy and Nutrients)
The third S is where a meaningful part of your biomarker picture lives. Your brain runs on a continuous supply of glucose, oxygen, omega-3 fatty acids, B vitamins, and a long list of micronutrients. Deficits in any of these can quietly compromise function for years before they show up as symptoms. When these markers are at optimal levels, they actively protect your brain, often for decades.
The first place to look is diet. What you eat every day is the primary driver of whether your brain gets what it needs. Targeted supplementation comes second, once you know where the gaps actually are.
The biomarkers we look at first in the Blueprint panel are homocysteine, vitamin D, vitamin B12, ferritin, and folate. These are the ones most likely to flag a nutrient supply problem before you feel it. And the fix is usually targeted, not maximal. Most clients don't need fifteen supplements, they need the right two or three, chosen based on what their labs actually show.
What you can do this week: If you haven't had a full brain-health panel in the past year, that's where to start. A nutrient gap rarely shows up in isolation, and the right intervention depends on seeing how everything fits together.
Why All Three Matter Together
The argument the book makes is that the components that support brain health aren't a long list of individual variables, they're an integrated network.
Stimulation without sleep doesn't give the brain time to consolidate. Sleep without nutrient supply leaves the brain trying to do its overnight work without raw materials. Nutrient supply without stimulation gives the brain everything it needs to grow but no reason to.
This is consistent with what BetterBrain's coaches see in practice. Clients who work hard on one of the three but ignore the others tend to plateau. The ones who address all three see the biggest shifts in biomarkers, cognitive scores, and how they actually feel.
The Bottom Line
The Stimulated Mind is the best communication of modern brain science available today, worth reading whether you're at the beginning of thinking about brain health or several years into a protocol.
Working with a BetterBrain coach to address all three Ss, across all 11 practices, is how you turn a framework into measurable results.
hs-CRP: The Biomarker Most Likely to Flag Silent Inflammation in Brain Health
If you have ever had a routine blood panel, you have probably seen "CRP" on the list. What you may not have seen is "hs-CRP," which sounds like the same test but is not. The difference matters a lot for brain health.
This piece walks through what hs-CRP measures, why it shows up in almost every BetterBrain protocol, and what to do if yours is elevated.
What hs-CRP measures
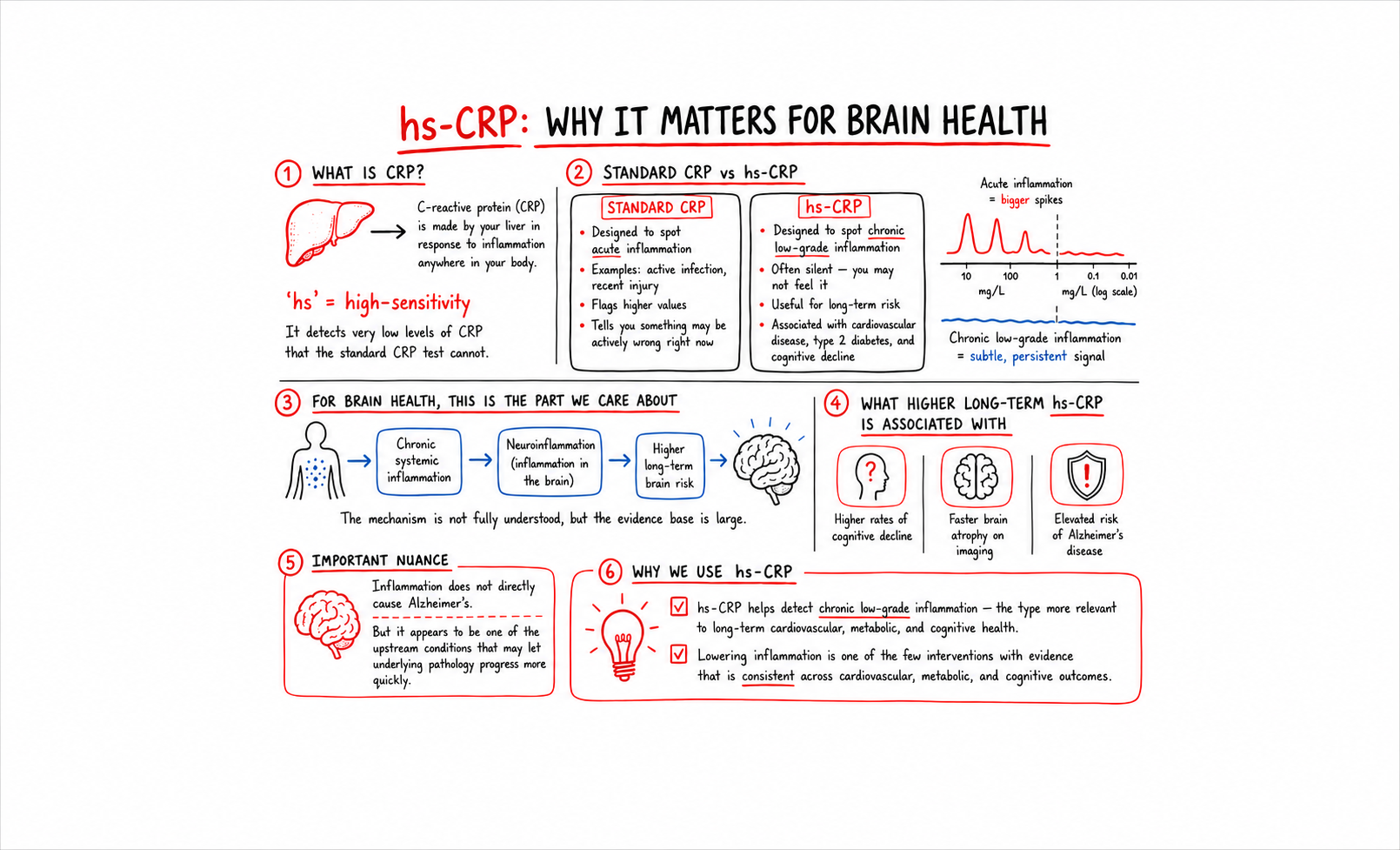
C-reactive protein is made by your liver in response to inflammation anywhere in your body. The "hs" stands for "high-sensitivity," which means the test can detect very low levels of CRP that the standard CRP test cannot.
This distinction sounds technical but it is the whole reason we use hs-CRP and not standard CRP. Standard CRP is designed to spot acute inflammation, like an active infection or a recent injury. The values it flags are high enough to indicate something is actively wrong right now. hs-CRP is designed to spot chronic low-grade inflammation, the kind that does not feel like anything but is associated with long-term risk for cardiovascular disease, type 2 diabetes, and cognitive decline.
For brain health, the chronic low-grade version is the one that matters.
Why this matters for your brain
Chronic systemic inflammation is associated with neuroinflammation, the inflammatory state of the brain itself. The mechanism is not fully understood, but the body of evidence is large. People with higher long-term hs-CRP have higher rates of cognitive decline, faster brain atrophy on imaging, and elevated risk of Alzheimer's disease.
Inflammation does not directly cause Alzheimer's. But it appears to be one of the upstream conditions that lets the underlying pathology progress more quickly. Lowering it is one of the few interventions where the evidence is consistent across cardiovascular, metabolic, and cognitive outcomes.
What the numbers mean
- Optimal: under 1.0 mg/L
- Borderline: 1.0 to 3.0 mg/L
- High: above 3.0 mg/L
Most standard labs flag a result only when it crosses 3.0 mg/L or higher. The 1.0 to 3.0 range is where a meaningful number of clients are quietly running elevated. Their primary care has waved it off as "in range." For brain health purposes, it is not.
The biomarkers that pair with hs-CRP
A single hs-CRP value is informative but more useful in context. The markers to look at alongside it:
Homocysteine. Elevated homocysteine is associated with both inflammation and methylation problems. If hs-CRP and homocysteine are both elevated, the inflammation is likely driven in part by nutrient gaps.
ApoB and Lp(a). Cardiovascular markers. Elevated hs-CRP plus elevated ApoB is a particularly bad combination for vascular brain health.
HbA1c and Fasting Insulin. Metabolic markers. Glycemic dysfunction drives systemic inflammation. If hs-CRP is elevated, look here next.
Ferritin. Iron storage. Elevated ferritin can indicate underlying inflammation, separate from iron status.
The picture you assemble from these markers tells you whether the inflammation is metabolic, vascular, nutrient-driven, or something else.
What to do about it
The interventions that consistently move hs-CRP overlap with the interventions that consistently move long-term cognitive trajectory. Sleep, glycemic control, omega-3 status, dental health, gut health, and visceral fat reduction are all associated with lower chronic inflammation over time. None of them are quick fixes. All of them compound.
For BetterBrain clients with elevated hs-CRP, the coaching protocol usually starts with the highest-leverage area their panel reveals. A client whose hs-CRP is elevated alongside high HbA1c starts with glycemic control. A client whose hs-CRP is elevated alongside high homocysteine starts with methylated B-complex and a closer look at folate, B12, and B6 intake. The technique is to follow the panel.
Find out where you stand
hs-CRP is one of the most useful brain-health markers in routine bloodwork, and one of the most commonly missed. If you have not had a high-sensitivity version of CRP measured in the past year, it is worth checking.
BetterBrain Blueprint covers hs-CRP alongside 50+ other markers and starts at $89 with insurance.
.png)
The Essential Techniques our coaches keep recommending for brain health
We use the term Essential Techniques inside BetterBrain a lot. Each BetterBrain Practice (Move, Sleep, Eat, De-Stress, and so on) is made up of specific techniques, and the Essential Techniques are the ones our panel of clinical advisors identified as the techniques with the greatest evidence and broadest applicability.
These are not techniques for a specific kind of client. They are the techniques worth considering for almost everyone thinking about long-term brain health, regardless of starting point, age, or risk profile. About 15 to 20 percent of the techniques in our library are Essential. The other 80 to 85 percent are context-dependent, applied when a client's panel or situation calls for them. A coach builds a personalized action plan by looking across the whole library, deciding which Essentials to elevate first and which context-dependent techniques to layer in. The Essentials are the foundation underneath every plan.
We asked some of our coaches what trends they are seeing across the clients they work with, and which Essential Techniques those trends keep pointing back to.
The post-meal walk (Move Practice)
Maggie works with clients across the metabolic-health side of our client base. The trend she keeps seeing: HbA1c and fasting insulin numbers creeping into pre-diabetic ranges, often without the client realizing it. Many of them are exercising, but most of them are not walking after meals.
"Ten minutes after each meal. That is the rule I get the highest compliance on, because nobody can argue they don't have ten minutes. And it does more than people expect."
This is one of the Essential Techniques in our Move Practice because the evidence is broad and the bar to entry is low. A short walk after eating blunts the post-meal glucose spike. Repeated over months, it is one of the most reliable ways we have seen to shift HbA1c, fasting insulin, and the metabolic conditions that drive midlife brain atrophy. The cost is nothing, the schedule disruption is minimal, and the long-term payoff compounds. It is essential because it works for almost everyone.
Consistent wake time and morning light (Sleep Practice)
Emily works with a large share of our clients who came to BetterBrain because of family history of dementia. The trend she keeps seeing: anxious clients arriving with long supplement lists, wanting to talk about pTau-217 and APOE4, while sleeping six or fewer hours a night.
"One night of four hours isn't really the question. The question is why someone is typically sleeping four or five hours at most. Patterns matter. What we identify from the first visit and where we end up is more than one night of poor sleep. Sleep is the foundation. Exercise goals, stress management, eating, they all land once sleep patterns are optimized."
The Essential Technique Emily points to first is in our Sleep Practice: a consistent wake time paired with morning light. The reason this is essential for almost everyone is the glymphatic system. Sleep is the period during which the brain runs its only clearance system, including the clearance of amyloid. A consistent wake time anchors the circadian rhythm, and morning light reinforces it. The evidence is strong, the intervention is free, and it works for clients in their 30s and their 70s.
Strength training (Move Practice)
Wendy works with many of our clients in their late fifties and sixties. The trend she keeps seeing: clients who are doing aerobic exercise faithfully, often three or four days a week, and skipping strength training entirely.
"I'm flexible with many aspects of a health plan, but strength training is one area I strongly encourage people not to overlook. The research connecting muscle mass and brain health after 50 is incredibly compelling, and maintaining strength now can have a major impact on long-term health and quality of life."
Strength training is another Essential Technique in our Move Practice. The reason it is essential, not optional: muscle is the primary site of glucose disposal in the body, the pathways linked to neurogenesis are responsive to resistance training, and sarcopenia is one of the strongest predictors of cognitive decline in older adults. The evidence supports two sessions a week, moderate intensity, sustained for at least six months. Bodyweight work and resistance bands are enough to start. The technique is essential because everyone past 30 is slowly losing muscle, and the cost of skipping it is too high.
Methylated B-complex (Supplement Practice)
Another trend we keep seeing across our client base: people arriving with homocysteine in the 11 to 14 range, told by their primary care that it is fine. The gap between what is flagged at most labs and what is optimal for brain health is one of the cleanest examples of where our framework differs from standard care.
The optimal range for homocysteine is under 9 μmol/L. Most labs flag a result only above 15. The 9 to 14 range is where a meaningful number of clients are quietly carrying elevated risk that has been waved off. A methylated B-complex moves the marker for the majority of clients within three months, and the cognitive payoff is real.
The Essential Technique in our Eat Practice is targeted methylated B-complex supplementation. The reason this is essential for almost everyone has to do with the underlying biology. Homocysteine is cleared through methylation pathways that depend on the active forms of folate, B12, and B6. A significant portion of the population carries variants of the MTHFR gene that reduce how well the body converts standard folic acid into the active form. Methylated B-complexes deliver the active forms directly. For anyone over 40 thinking about long-term brain health, this is one of the highest-leverage interventions available.
What the pattern reveals
Across our coaches with different specialties and different client populations, the same Essential Techniques keep coming up. These are the techniques that consistently move the needle, regardless of who is doing them. What our coaches actually do day to day is build action plans that span the full technique library, prioritizing among the Essentials and layering in the context-dependent techniques that fit each client's panel and life.
The Essentials are universal. The action plan is personal.
Find out where to start
If you'd like a quick read on which Essential Techniques to prioritize based on what you are already doing, take the free Essential Scan. Open to anyone, whether you're already a BetterBrain client or just starting.
If you'd like a deeper personalized action plan, BetterBrain coaching pairs you with a Brain Health Coach who builds the plan with you. Coaching is covered at $0 for 92% of approved clients with qualifying insurance.

Visceral Fat and the Brain: What 16 Years of Data Actually Show
A study just landed in Nature Communications that reframes how to think about midlife weight loss and brain health. Researchers followed 533 adults for up to 16 years after they completed lifestyle interventions, then scanned their brains and tested their cognition. The finding: it wasn't weight loss that predicted slower brain atrophy and better cognitive scores years later. It was sustained loss of visceral fat specifically.
This matters because most people, and most doctors, still track weight on a scale. The number on the scale lumps together fat, muscle, water, and where on the body the fat actually sits. The new data suggests that for brain health, where the fat is matters more than how much of it there is.
What the study found
The research, called the Follow-Interventions-Trials (FIT) project, pulled participants from four earlier 18 to 24 month lifestyle randomized trials. The average age at follow-up was 61. Each participant had abdominal MRI, brain MRI, and Montreal Cognitive Assessment (MoCA) testing 5 to 16 years after their original intervention.
Three findings stood out. Lower long-term visceral fat exposure, calculated across baseline, post-intervention, and follow-up, independently predicted higher cognitive scores. Visceral fat loss during the intervention period predicted higher brain volumes years later, independent of overall weight loss. And among the participants who had three full sets of scans over the years, lower long-term visceral fat was associated with a slower rate of brain atrophy.
The same patterns were not observed for subcutaneous fat, the kind that sits under the skin and shows up on a pinch test. Visceral fat, the deeper fat surrounding the organs, was the variable that mattered.
The proposed mechanism is glycemic. Visceral fat is metabolically active. It secretes inflammatory signals and contributes to insulin resistance. Both of these are increasingly understood as drivers of cognitive decline. When visceral fat goes down, glycemic control improves, and the brain appears to benefit downstream.
Why this changes how we think about midlife weight
Most people who decide to lose weight in their fifties do not distinguish between subcutaneous fat, visceral fat, and muscle. Many lose all three. Losing muscle in midlife is a problem on its own. Losing subcutaneous fat without losing visceral fat is largely cosmetic. Losing visceral fat appears to be the part that actually protects the brain.
This also reframes "skinny fat." A person can have a body mass index in the normal range and still carry significant visceral fat. The scale will not flag this. A waist measurement, a DEXA scan, or abdominal imaging will.
For anyone in their 40s, 50s, or 60s thinking about brain health, the practical question is no longer "should I lose weight." It is "what is my visceral fat doing, and what is actually moving it."
What you can do
Three things tend to move visceral fat without requiring dramatic restriction.
The first is reducing refined carbohydrates and added sugars. Visceral fat is more responsive to insulin signaling than subcutaneous fat. Lowering postprandial glucose spikes is associated with reduced visceral fat over time.
The second is consistent moderate-intensity movement, especially after meals. A 10 to 15 minute walk after eating blunts the post-meal glucose curve. Repeated over months, this contributes meaningfully to visceral fat reduction.
The third is strength training, which we covered last week. Muscle is the primary site of glucose disposal in the body. More muscle means better glycemic control, which means less visceral fat accumulation.
The biomarkers that respond, and the ones we look at first with members, are HbA1c (your average blood sugar over three months), fasting insulin, and the broader metabolic panel that looks at lipids and liver function. These shift before the scale shifts. They tell you whether the metabolic conditions that drive visceral fat are improving.
The bottom line
The next time someone tells you to lose weight for your brain, the more useful version of that advice is to lose visceral fat for your brain. The number on the scale was always a poor proxy for what is happening inside the body. The new research makes that clearer.
If you are already a BetterBrain member, your most recent HbA1c, fasting insulin, and metabolic panel results are in your dashboard. Worth a fresh look in light of this.
If you have not yet started, these markers are part of the BetterBrain Essentials Panel we look at first.
Get immediate insights with a 3 minute assessment
Start now.png)
GreyMatters
Harnessing Heart Rate Variability for Brain Health
The intricate dance between our heart rate and brain function is more influential than we might think. Recent studies reveal that heart rate variability (HRV)—the measure of variations between individual heartbeats—affects our brain health, decision-making abilities, and even our emotional regulation. HRV is a physiological metric that we can train ourselves to improve, and its connections to the brain make HRV training a promising technique for dementia prevention and enhancing cognitive function.
Understanding the Heart-Brain Connection:
While your heart rate is the average number of beats per minute, HRV is the difference in length between individual heartbeats.

HRV is not just a measure of heart health - it reflects the health and balance of the autonomic nervous system (ANS), which is responsible for involuntary body functions. In particular, HRV serves as a key indicator of the interaction between the two components of the ANS: the sympathetic (fight or flight) and parasympathetic (rest and digest) nervous systems. Interestingly, there is a two-way feedback system between these nervous systems and the heart. The signals from the sympathetic and parasympathetic influence heart rate, and heart rate regulates the balance of these two systems. By exerting an influence on the ANS, heart rate variability helps regulate emotions and stress responses. In general, higher HRV is associated with better control over decision-making processes, emotional responses, anxiety, and social behaviors1.
Booting your HRV
Common HRV training protocols call for biofeedback, which is a fancy way of saying you need a sensor to measure your heart rate variability so you can improve it. HRV training involves guided exercises such as paced breathing while looking at real-time heart rate data to learn to consciously control heart rate variability. This is what makes it different from techniques like yoga or meditation - their focus is commonly to achieve a balanced state, whereas the goal of HRV training is to modulate physiological responses.
This technique not only promotes a balanced state but also has long-lasting effects on both mental and physical health. Thanks to the heart-brain connection, HRV training leads to improved emotional regulation and stress management. Although different training regimens exist, just five minutes of HRV training twice a day can significantly enhance control over the heart and reduce anxiety levels during stressful periods2. Critically, the benefits of HRV training extend far beyond mood and feeling: they also correlate with enhanced executive functions like planning, problem-solving, and resisting unhealthy impulses1. In fact, the benefits of this training can persist, with improvements seen even 12 weeks after stopping the training1.
Tying back to dementia
Thanks to its influence on stress response, cognitive function, healthy behaviors, and cardiac health, it’s no surprise that higher HRV is associated with stronger resilience against cognitive decline2,3. Since the simple daily practice of HRV biofeedback training can improve your HRV, we can think of it as a valuable tool to help delay the onset and progression of dementia. It's a clear testament to the power of our bodies' interconnected systems, and a reminder that taking care of our heart is as much about our mind.
Where to start with HRV training
- Choose a tracking device: the first step is to make sure you have the right equipment to measure your heart rate variability. Because you are measuring the time between individual heartbeats, you need a particularly sensitive device. Although some common wearables like the Apple watch or Whoop claim to measure HRV, it’s better to opt for a specialized chest strap like the Polar H10 which can connect to your other wearables.
- Visualize your data: once you have a solid device, use an app like Elite HRV or Welltory (both of which have a free version available) so that you can visualize your HRV in real time. These apps also come with a wealth of additional insights that can help you fine tune your training.
- Start training: you can find guided training sessions either through apps like Elite HRV or through online courses provided by organizations like the HeartMath Institute. YouTube also has a number of guided HRV routines you can try, such as this one from the Huberman Lab show.
- Learn more: The Peter Attia Drive podcast has an episode that dives deep into HRV so you can learn more about how it works and how it can help you.
Metabolic Syndrome as a Gateway to Dementia
It’s a well-known fact that Alzheimer’s disease is closely linked to metabolic health, to the point that some experts have begun to refer to it as Type III Diabetes. But what many people don’t know is that poor metabolic health is a strong risk factor for dementia long before it progresses to diabetes, even for people without a family history.
Decoding metabolic syndrome
Before you get diagnosed with diabetes, your body goes through a number of changes. Cells in your body become desensitized to insulin, which usually tells them to absorb sugar from your bloodstream. This results in chronically elevated blood sugar and in turn starts causing problems for your heart, liver, brain, and other organs. This pre-diabetic phase is called metabolic syndrome, and it affects ~25% of adults worldwide, including 40% adults aged 60+ in the U.S. Most of them do not know that metabolic syndrome is a health risk.
Metabolic syndrome is diagnosed when an individual has three or more of the following:
- High triglycerides (≥150 mg/dL)
- Elevated blood pressure (≥130 mmHg systolic or ≥85 mmHg diastolic) OR use of antihypertensive medication
- High fasting glucose (≥100 mg/dL OR use of glucose lowering medications)
- Low HDL cholesterol (<40 mg/dL in men; <50 mg/dL in women OR use of lipid-modifying medication)
- Abdominal obesity (waist circumference ≥102 cm for men and ≥88 cm for women)
It’s worth noting that hemoglobin A1c (HbA1c), a common marker for diabetes, does not feature on this list. Although a doctor won’t use A1c to diagnose metabolic syndrome, it’s still an important marker to keep track of your metabolic health.
Connecting metabolic syndrome to brain health
A large retrospective study1 analyzed data from 175,000 participants over a period of 15 years. Participants were aged 60+ and represented a variety of sociodemographic, lifestyle, and genetic backgrounds. With regards to the metabolic syndrome diagnosis criteria listed above, the study found that:
- Having three conditions increases dementia risk 12%
- Having four to five conditions is associated with an even stronger risk
- The link between metabolic syndrome and dementia is particularly strong in individuals who do not carry the APOE ε4 allele (typically, these are individuals with a lower risk of dementia)
Taking action
The first step is to know where you stand. It’s important to establish a baseline by measuring metabolic markers in your blood and potentially using a continuous glucose monitor (CGM) to see how your blood sugar reacts to your daily habits. This will help you make an informed decision on how to approach your metabolic health.
Metabolic health is strongly tied to your lifestyle - particularly your diet, physical activity, and sleep. There’s also several different drugs, like statins or ACE inhibitors, available to help manage symptoms. However, this post isn’t meant to serve as a meal plan or exercise sheet. Instead, we’ve put together a list of hacks that we think can make a difference even if you haven’t fully optimized your health.
- Drink a tablespoon of vinegar ~20 minutes before a meal. This helps avoid spikes in your blood sugar.
- Go for a walk after meals, especially if those meals are heavy on carbs (e.g., pasta, potatoes, bread). This helps your muscles absorb glucose more efficiently.
- Perform at least 10m of vigorous exercise per day. Raising your heart rate (e.g., through a short HIIT session) helps boost your insulin sensitivity, which keeps blood sugar low.some text
- Exercise is most effective at reducing blood sugar spikes when done within an hour before or after a meal
- Eat your carbs last. Start your meal by eating vegetables (which are high in fiber), then eating proteins and fats, and finally moving to carbs. This helps slow the absorption of sugar into your bloodstream, and in turn reduce sugar spikes.
Small steps add up
Although the hacks mentioned above aren’t meant to replace a healthy lifestyle, they can help you make an immediate improvement in your metabolic health and kickstart your dementia prevention efforts. Remember - working on your metabolic health isn’t just about preventing diabetes, it’s about safeguarding your cognitive health.
Actions to consider
- Measure your metabolic markers. Some of these you may get on your annual physical (e.g., HbA1c, HDL-C, LDL-C, glucose, triglycerides, insulin). Others are less common (e.g., Lp(a), ApoB). Most importantly, don’t settle for just ok. These markers are worth optimizing. All the tests mentioned above are part of the 50+ biomarkers tested during your BetterBrain Essentials blood draw.
- Consider using a CGM to get a more accurate view of how your body processes sugar. Using a CGM, you can observe the effects of what you eat and your lifestyle on your blood sugar in real time, which can help inform the daily choices you make. We love the Dexcom G7, which may be challenging to buy over-the-counter but can be bought for cheaper through Signos.
- Learn more about homocysteine on the Peter Attia Drive podcast #252. This episode covers a wide variety of topics related to brain health, and links many different risks and possible interventions to metabolic health.
Rapamycin: Revolutionizing Alzheimer's Prevention?
In the 1960s, researchers on Easter Island were investigating local indigenous peoples’ claims that the soil has healing properties. After testing various soil samples, the researchers isolated a small molecule they believed was responsible for the effects. They named it rapamycin5, after the traditional name for the island, Rapa Nui. Since its discovery, rapamycin has been used in various settings, from an antifungal agent to more recently a beacon of hope in anti-aging medicine. Additionally, it is showing promise in extending lifespan and preventing neurodegenerative diseases such as Alzheimer’s.
From anti-rejection med to longevity enhancer
The transition from an antifungal to a potential longevity drug has been intriguing. Rapamycin, approved in 1999 for its immunosuppressant qualities, is still commonly used in kidney transplants to prevent organ rejection. However, a 2014 study1 on older adults revealed a paradox: at much smaller doses, rapamycin boosted the immune response to flu vaccinations, despite their age-related weakened immune function. This unexpected enhancement suggests that rapamycin might have broader applications for disease prevention in older adults, potentially making it a valuable tool in combating age-related declines in the human immune system.
How rapa works
To understand how rapamycin works, it’s important to understand the molecule that it targets: a cellular receptor named mTOR. mTOR is present in nearly all cells in the human body and is responsible for mediating pathways that regulate cell growth, metabolism, and survival. Inhibiting mTOR completely is catastrophic - it prevents cells from making energy, eventually leading to their death. However, partial inhibition means that mTOR has a harder time forming a cluster with other proteins, which makes the cell act as if it's not getting enough food. This starts a process where the cell breaks down unneeded or damaged parts, like proteins that aren't folded correctly, which can otherwise impair the cell’s ability to function. This leads to improved cellular survival and resilience and is particularly relevant to brain health since one of the main features of Alzheimer’s is the accumulation of misfolded amyloid beta protein plaques in neurons.
The partial inhibition of mTOR therefore shows potential for slowing down the progression of Alzheimer’s disease and improving the survival rate of neurons. Animal studies2,3 suggest that rapamycin may help mitigate or improve many of the pathologies associated with Alzheimer's disease and potentially restore cognitive function.
Growing evidence yet limited human trials
While animal studies have robustly demonstrated lifespan and healthspan extensions—with remarkable outcomes like a 20-30% increase in the lifespan of mice4—human data remains scarce. The gap in human trials can be largely attributed to the fact that rapamycin use for longevity is considered “off-label”. This means that the Federal Drug Administration (FDA) has not yet approved rapamycin for this use, which diminishes incentives for comprehensive research funding. However, the evidence from animal studies across a variety of species strongly suggests a significant potential for rapamycin in anti-aging treatments.
Rapamycin’s mainstream use
As mentioned earlier, the FDA has only approved rapamycin for use as an immunosuppressant. It’s important to recognize that rapamycin use for longevity is still considered experimental and will not be reimbursed by insurance. Because the FDA hasn’t established guidelines around its use, there is no single accepted protocol for rapamycin dosage. Given the drug’s complex effects, the risk of experiencing side effects is real. Nonetheless,many individuals already use rapamycin “off-label” under the supervision of a physician for its longevity benefits. This is a perfectly legitimate use of the molecule, even though there is a lot we have yet to learn.
A promising option for the future
Rapamycin offers a compelling glimpse into the future of longevity and neuroprotection. Although its journey from a soil sample to a potential anti-aging miracle has been gradual, the promise it holds could change the landscape of preventive health. As research continues, both the medical community and potential users must weigh the benefits against the uncertainties of translating animal model successes to human health outcomes.
Learn more
Listen to the Peter Attia Drive episode on rapamycin to learn more about the molecule, its history, how it works, and the most recent evidence on its effects.
Unlocking the Power of Omega-3 Fatty Acids
As the quest for effective Alzheimer’s prevention continues, recent studies1,2 underscore the profound impact of dietary choices on our brain health. One nutrient class consistently at the forefront of neuroprotective research is Omega-3 fatty acids, particularly Docosahexaenoic Acid (DHA) and Eicosapentaenoic acid (EPA). In this post, we explore how integrating DHA and EPA into your diet can play a crucial role in reducing the risk of Alzheimer's disease.
Fatty acids explained1
DHA and EPA are a major omega-3 fatty acid predominantly found in fish oils. They are called essential fatty acids, meaning that the human body cannot produce them on its own, so they must come from dietary sources. Make sure not to confuse omega-3s (like DHA and EPA) with omega-6s. These are a different class of fatty acids typically found in vegetable oils and nuts. They are much more common in most diets, and can promote inflammation when consumed in excess.
DHA and EPA are particularly important because the molecules are building blocks for neurons. This means that maintaining healthy levels of DHA and EPA supports neuronal membrane integrity, promotes healthy synaptic activity, and mitigates inflammation within the brain. Long-term, these fatty acids have been shown to help preserve cognitive abilities and delay the onset of dementia1.
Clinical insights on Alzheimer’s prevention
A growing body of research points to a direct correlation between DHA and EPA intake and a reduction in the risk for Alzheimer's. Animal studies provide compelling evidence, showing that diets rich in DHA can significantly reduce the formation of amyloid plaques, which are closely linked to Alzheimer’s pathology1.
Furthermore, in human epidemiological research (research that investigates the distributions and determinants of health-related events in populations), increased consumption of DHA through dietary sources like fish has been associated with lower incidence rates of Alzheimer’s, suggesting its significant protective effect. One study3 found that people with the highest levels of DHA had a 49% lower risk of developing Alzheimer's disease compared to those with the lowest levels. This means that those in the top 20% were about half as likely to get Alzheimer's as those in the bottom 20%. Additionally, increasing DHA levels from the lowest group to the highest group was predicted to give an extra 4.7 years of life free from Alzheimer's disease.
Other studies have concluded similar results, showing a 47%5 reduction in risk, though there is debate about when this effect may occur. The consensus is that DHA supplementation is most effective when started early, before symptoms get classified as dementia6.
Increasing your omega-3 intake
There are two main ways to make sure you’re getting enough DHA and EPA - either making conscious dietary choices4 or taking supplements. From the diet side, fatty fish are an excellent source of omega-3s. Typical guidance recommends eating fish like salmon, mackerel, herring, or halibut at least 3 times per week. It’s worth noting that chia seeds and flax seeds are also excellent sources of omega-3s. Predatory fish like tuna are also good sources of EPA and DHA, but be careful not to consume them too often since they also contain high levels of mercury.
Fish oil supplements can be another great way to increase your intake of omega-3s - if you carry the APOE4 gene, supplementation is particularly important since you may have more trouble absorbing dietary omega-3s. However, it’s important to recognize that not all supplements were created equal. Specifically, not all brands will have the same purity of fatty acids, and not all will contain sufficient levels of DHA and EPA. Here are some things to look out for to make sure you are getting high quality fish oil:
- High amounts of DHA and EPA per serving (at least 500mg combined per serving)
- Minimal additives in the ingredients other than the oil and capsule contents
- Packaged in dark containers to protect the oil from light
A Step Towards Cognitive Longevity
Embracing a diet that includes adequate amounts of DHA and EPA can significantly contribute to brain health and potentially decrease the risk of Alzheimer’s. Start by evaluating your current dietary habits and consider how you might improve your omega-3 intake, ensuring your brain remains vibrant and healthy well into later life.
Where to get started
- Measure your blood omega-3 index to learn your current EPA and DHA levels. This is one of the 50+ biomarkers tested during your BetterBrain Essentials blood draw.
- Eat at least 3 servings of fatty fish (e.g., salmon, mackerel) per week, but make sure not to overdo your intake of predatory fish like tuna.
- Consider using fish oil supplements to increase your EPA and DHA intake. We recommend Carlson’s fish oil, which is available at a discount with a BetterBrain membership.
The Rise of Amyloid Blood Tests
The Landscape of Alzheimer's Biomarkers
When it comes to assessing the risk of cardiovascular disease, we have straightforward biomarkers such as ApoB (LDL) and blood pressure which can predict risk fairly accurately. However, the realm of neurodegenerative diseases like Alzheimer's is a lot more messy. For years, researchers and clinicians have depended PET scans or cerebral spinal fluid (CSF) for analyzing biomarkers like amyloid and tau proteins. But these procedures are expensive ($5-10K in the case of PET) or invasive (CSF requires a lumbar puncture), making them impractical for widespread use.
Enter blood amyloid tests, a relatively new but promising diagnostic aimed at solving this problem.
What Are Blood Amyloid Tests and How Do They Work?
As the name suggests, these tests measure the concentration of various amyloid beta proteins in the blood (and sometimes tau as well) as a proxy for amyloid deposition in the brain. While the scientific community continues to debate whether amyloid pathology is a root cause of Alzheimer's disease or merely a symptom of other underlying brain pathologies, there is a clear association between the extent of amyloid presence in the brain and the manifestation of the disease.
One of the original commercially available tests was PrecivityAD by C2N. This test needs to be ordered by a physician and was designed to predict the likelihood of Alzheimer's Disease (AD) pathology by analyzing a few key factors:
- The ratio of two variants of amyloid beta proteins, specifically amyloid beta 42 and amyloid beta 40
- The ApoE variant of the patient
- The age of the individual
By amalgamating these variables, the test attempts to gauge the probability of a positive PET scan. While it's too early to draw any definitive conclusions, there are two primary reasons why looking at this data could be valuable:
- Comprehensive Risk Assessment: The test results can be used in combination with other factors like family history, genetics, metabolic health, vascular health and cognitive testing to assess the overall risk.
- Monitoring Interventions: The score could be used as a dynamic indicator to monitor the effectiveness of steps taken to mitigate Alzheimer's risk. If the score decreases, it suggests that the ratio of amyloid beta 42 to amyloid beta 40 has changed favorably and thus risk has been reduced.
Since then, C2N launched a second generation version of the tests, PrecivityAD21, which accounts for serum tau concentration for additional accuracy. In August of 2023, Quest launched a direct-to-consumer version of the test that does not require physician ordering. While the test is not quite as accurate as C2N in predicting a positive PET, it comes at a materially lower cost - $400 as of the date of this writing.
Applicability: Who Should Consider blood amyloid tests?
According to medical experts, the test should be reserved for those at high risk of developing Alzheimer's, as its sensitivity and specificity are still not entirely understood. The key term here is "pre-test probability." The higher the pre-test probability, the more reliable the test becomes in predicting a positive or negative outcome.
Final Thoughts
The emergence of amyloid (and tau) blood tests is an exciting development in the field of Alzheimer's research and prevention. Although not a complete solution, they do provide an additional layer of information that can potentially enhance our ability to serve people at risk of developing disease. As our grasp of amyloid biomarkers improves, these tests could become integral parts of a broader, more nuanced approach to diagnosis and risk assessment.
Update April 19, 2024
Roche, in collaboration with Eli Lilly, has launched the Elecsys pTau-2172 blood test, which has recently received breakthrough device designation from the FDA. This means it was recognized as an effective tool for diagnosis, and is a critical milestone in how we identify Alzheimer's Disease. This test targets the tau protein pTau-217 and has the unique ability to distinguish AD from other neurodegenerative diseases. This is particularly important given that clinical AD diagnoses often lack sensitivity and specificity. It’s all the more since over half of patients with cognitive impairment remain undiagnosed or incorrectly diagnosed. This advancement promises to enhance early diagnostic accuracy and significantly improve intervention strategies for AD, particularly as global dementia figures are projected to rise sharply by 2050. pTau-217 is now available as an add-on service with BetterBrain.
Saunas and Alzheimer's: Hot Topic or Just Hot Air?
For centuries, saunas have been lauded for their supposed health benefits, from improved cardiovascular function to detoxification. The recent trends around longevity seem to have revitalized the use of saunas, now considered a popular "health hack". But could spending time in these heated chambers also benefit your brain? Recent research suggests that sauna use might indeed play a role in mitigating the risk of Alzheimer's disease. In this article, we'll explore the scientific evidence behind this claim and consider how sauna use may impact your brain health.
The Connection Between Saunas and Alzheimer's Disease
The Finnish Study
A study from Finland has brought attention to the potential benefits of saunas for brain health. According to the 2,315 person study1, men who used a sauna 4-7 times a week showed a 65% reduced risk of Alzheimer's disease compared to those who used it once a week. Although the study mainly focused on men and thus requires further exploration for generalization, the findings are promising - 65% is a staggering number. If true, this would imply we could cut Alzheimer's prevalence from 6 million to 2 million in the US if only everyone used the sauna daily!
The Underlying Mechanisms
Scientists have proposed several mechanisms through which saunas may benefit the brain. One suggestion is that saunas can significantly improve sleep quality and time in deep sleep, which improves the brain's ability to clear toxic proteins. Moreover, heat stress activates heat shock proteins that can repair damaged proteins, which may play a role in neurodegenerative diseases like Alzheimer's. Lastly, saunas may improve various markers of vascular function, such as blood pressure and blood circulation, known risk factors for Alzheimer's.
Caveats and Considerations
First, the impact was more muted for those who used the sauna only 2-3 times a week (~22% risk reduction). Additionally, while the Finnish study shows a correlation, and certainly attempted to control for relevant variables, it is always very challenging to prove causation in retrospective studies.
Conclusion
The notion that saunas could "incinerate" your Alzheimer's risk is captivating, they should not be viewed as a standalone solution. While promising studies hint at a beneficial correlation, saunas are not a guaranteed prevention method for Alzheimer's. However, given their other health benefits and the intriguing data suggesting a potential role in brain health, saunas could be a worthwhile addition to your wellness routine. Plus, who doesn't enjoy an intense sauna session followed by a cold plunge or shower?