GreyMatters
Educational articles, BetterBrain resources, latest in brain health, and news about us. Written for you, with expertise (and love).

Strength Training and Brain Health: What 6 Months of Lifting Does to Your Hippocampus
Strength Training and Brain Health: What 6 Months of Lifting Does to Your Hippocampus
Aerobic exercise gets most of the brain-health attention. The cardiovascular benefits are well-documented, the GPLD1 pathway connecting movement to blood-brain barrier repair is real, and almost every brain health protocol recommends it.
But a body of research has been quietly building on a different type of exercise entirely. And a comprehensive 2025 network meta-analysis just made the case for strength training impossible to ignore.
What the research found
The analysis, published in Frontiers in Aging Neuroscience, pulled data from dozens of randomized controlled trials involving cognitively healthy older adults. When researchers compared aerobic exercise, resistance training, mind-body practices like yoga, and combined programs for their effect on cognitive function, resistance training produced the strongest overall effect on global cognition. The effect size was considered moderate to large in cognitive research, where meaningful improvements are notoriously difficult to achieve.
A parallel 2025 systematic review went further. It examined actual brain imaging alongside cognitive testing. The findings: at least two resistance training sessions per week, sustained for at least six months, were associated with measurable increases in cortical thickness in two critical brain regions.
The hippocampus, your brain's primary memory formation center. And the prefrontal cortex, involved in planning, complex reasoning, and self-control. These are precisely the regions most vulnerable to aging and most associated with early cognitive decline.
These weren't just improvements in test scores. These were structural changes in brain tissue, visible on MRI scans. Six months of consistent strength training literally changed the physical structure of participants' brains.
How it works
The mechanisms connecting resistance training to brain health are distinct from aerobic exercise benefits, which is exactly why both matter.
When your skeletal muscles contract under load, they secrete signaling proteins called myokines into your bloodstream. One well-studied myokine, irisin, crosses the blood-brain barrier and has been shown to increase new brain cell formation and reduce neuroinflammation in research models.
Resistance training also improves insulin sensitivity in your muscles, contributing to better metabolic health throughout your body. Given that brain insulin resistance is increasingly understood as a central mechanism in Alzheimer's disease, this metabolic pathway from strength training to brain protection isn't minor.
The exact dose the research supports
Frequency: At least two sessions per week. Some studies suggest three sessions produce greater effects, following a dose-response pattern.
Duration: Six months minimum for structural brain changes to appear on imaging. This isn't a quick fix. It's a sustained practice.
Intensity: Moderate intensity works best, approximately 50 to 70 percent of your maximum. In practical terms, this means lifting a weight you can complete 8 to 12 controlled repetitions with, where the final 2 to 3 reps require genuine effort.
Going through the motions with very light resistance doesn't appear to produce the same stimulus. The dose matters as much as the activity itself.
You don't need a gym membership to start. Bodyweight exercises (squats, push-ups, lunges), resistance bands, or even filled water bottles work. The goal is progressive challenge over time, gradually increasing difficulty as you get stronger.
Tracking whether it's working
Several markers respond to consistent strength training and give you objective evidence the work is paying off.
Insulin sensitivity: Resistance training improves how your cells respond to insulin. You can track this through fasting insulin and HbA1c, which shows your average blood sugar control over three months. Better insulin sensitivity is associated with better cognitive function.
Inflammatory markers: Consistent strength training reduces systemic inflammation. hs-CRP and homocysteine levels respond, giving objective evidence of the anti-inflammatory effect.
Metabolic health markers: Strength training improves multiple metabolic markers including glucose control, lipid profiles like VLDL-C, and overall metabolic function. These improvements happen through muscle-mediated pathways that complement what aerobic exercise does.
Seeing these numbers move is concrete evidence that the effort is producing real change.
The case for combining aerobic and resistance training
Aerobic exercise works through the GPLD1 pathway, where your liver releases protective signals during movement that repair your blood-brain barrier.
Strength training works through entirely different pathways: muscle-derived signaling proteins, improved insulin sensitivity, and hormonal changes that protect brain structure.
These are complementary, not redundant. Research on combined programs shows that doing both produces greater cognitive benefit than either alone. If you're already doing aerobic exercise regularly, adding just two strength sessions per week hits the research-backed minimum.
If you're curious where your insulin sensitivity, inflammation, and metabolic markers stand, BetterBrain's Blueprint testing covers all of them in a single panel, plus 40 more brain health markers.
Cholesterol and Your Brain: What You Actually Need to Know
Cholesterol gets a bad rap. For decades, we've heard that it clogs arteries and causes heart attacks. But here's what doesn't make headlines: your brain contains 25% of your body's total cholesterol despite making up only 2% of your body weight. As lipid expert Dr. Tom Dayspring puts it, "Cholesterol is almost certainly the most important molecule in the brain."
So how can cholesterol be both necessary for brain function and a major cardiovascular risk factor? The answer lies in understanding where cholesterol is, how it gets there, and what form it takes.
In this post, we're taking a deeper dive into cholesterol than usual. We'll break down what your cholesterol numbers actually mean, why the standard tests miss critical information, and how the cholesterol story connects cardiovascular health to brain health.
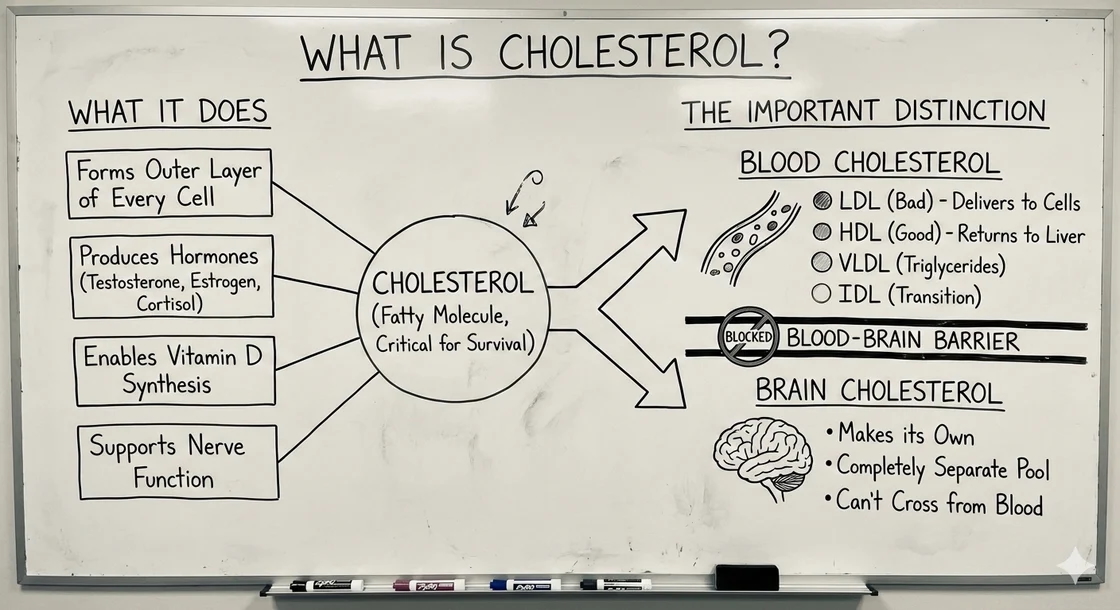
The Basics: What Is Cholesterol?
Cholesterol is a fatty molecule that serves critical functions throughout your body. It forms the outer layer of every cell, helps produce hormones (including testosterone, estrogen, and cortisol), enables vitamin D synthesis, and supports nerve function. Without cholesterol, you simply couldn't survive.
But there's an important distinction to make: "cholesterol" isn't one thing.
When we talk about cholesterol in the blood versus cholesterol in the brain, we're really talking about two separate systems that operate differently.
Blood cholesterol: Cholesterol travels through your bloodstream inside particles called lipoproteins. These particles come in different types:
- LDL (low-density lipoprotein): Often called "bad" cholesterol, LDL particles deliver cholesterol to cells throughout your body
- HDL (high-density lipoprotein): Called "good" cholesterol, HDL particles help transport excess cholesterol back to the liver
- VLDL (very low-density lipoprotein): Primarily transports triglycerides but also carries some cholesterol
- IDL (intermediate-density lipoprotein): A transition form between VLDL and LDL
Brain cholesterol: Your brain makes its own cholesterol and keeps it completely separate from blood cholesterol. The blood-brain barrier prevents cholesterol in your bloodstream from entering your brain. This means the cholesterol circulating in your blood and the cholesterol in your brain are part of two entirely different pools.
The Heart Risk: Why apoB Matters More Than LDL?
What is apoB?
ApoB (apolipoprotein B) is a protein found on the surface of all atherogenic (plaque-forming) particles, including LDL, VLDL, IDL, and Lp(a). Each particle contains exactly one apoB molecule, making apoB a direct count of total potentially harmful particles.
Why apoB beats LDL cholesterol?
Traditional LDL-C (LDL cholesterol) tells you how much cholesterol LDL carries, but not how many particles you have. Two people can have identical LDL-C but vastly different particle numbers and risk levels.
- Many small LDL particles (each carrying less cholesterol) = "normal" LDL-C but high particle count and high risk
- Fewer large LDL particles (each carrying more cholesterol) = higher LDL-C but fewer particles and potentially lower risk
ApoB counts every atherogenic particle regardless of size. This makes it the best single marker for cardiovascular risk.
What is the triglyceride connection?
Elevated triglycerides (often from insulin resistance) fundamentally alter lipid metabolism:
- VLDL becomes triglyceride-enriched
- Particles get remodeled into small, dense LDL
- ApoB particle count increases
- You can have "normal" LDL-C but dangerously high apoB
This is why metabolic health is critical for cardiovascular risk.
The Brain Side: Why Cholesterol Is Essential
While high apoB threatens your heart, brain cholesterol is absolutely essential.
Critical brain functions
- Myelin formation: Insulates nerve fibers for rapid signal transmission
- Synapse formation: Creates and maintains neuron connections
- Cell membranes: Every neuron needs cholesterol-rich membranes
- Neurotransmitter release: Regulates how neurons communicate
How the brain gets cholesterol
Astrocytes (brain cells) produce cholesterol and package it into brain-specific lipoproteins containing apoE (apolipoprotein E) for delivery to neurons.
The APOE genetic factor
- APOE ε2: Protective against Alzheimer's, better cholesterol handling
- APOE ε3: Most common, considered neutral
- APOE ε4: Increases Alzheimer's risk, disrupts brain cholesterol metabolism
Research from MIT shows APOE4 is associated with brain cells accumulating cholesterol abnormally rather than using it to make healthy myelin. This isn't about too much or too little cholesterol, but how effectively the brain uses it.
Cholesterol and Alzheimer's
Brain regions vulnerable to Alzheimer's show signatures of being "super cholesterol-hungry," as researchers describe it, constantly trying to produce and absorb cholesterol. When this system fails (especially with APOE4), neurodegeneration may follow.
The Paradox Resolved
In the bloodstream: High apoB drives atherosclerosis. Particles penetrate artery walls, oxidize, trigger inflammation, form plaques. Goal: Keep apoB low (<60-80 mg/dL) to prevent cardiovascular disease.
In the brain: The brain makes its own cholesterol independently. Blood cholesterol can't cross the blood-brain barrier. Goal: Support healthy brain cholesterol metabolism through metabolic health.
This separation means lowering blood cholesterol doesn't starve your brain. Your brain continues making what it needs regardless of apoB levels.
The Bottom Line
Cholesterol isn't inherently good or bad; context is everything. In your bloodstream, high apoB poses serious cardiovascular and cerebrovascular risks. In your brain, cholesterol is essential for structure and function.
The good news: these systems are separate. Lowering apoB to protect your heart doesn't harm your brain. In fact, protecting your cardiovascular system through better lipid management, metabolic health, and inflammation control also protects your brain.
Understanding which biomarkers matter empowers informed decisions. It's not about fearing cholesterol; it's about managing it intelligently.
Want to Understand Your Complete Lipid Profile and Genetic Risk?
BetterBrain includes apoB, advanced lipid testing, metabolic biomarkers, and APOE genetic testing for a complete cardiovascular and brain health picture.

Unlocking the Power of Omega-3 Fatty Acids
As the quest for effective Alzheimer’s prevention continues, recent studies1,2 underscore the profound impact of dietary choices on our brain health. One nutrient class consistently at the forefront of neuroprotective research is Omega-3 fatty acids, particularly Docosahexaenoic Acid (DHA) and Eicosapentaenoic acid (EPA). In this post, we explore how integrating DHA and EPA into your diet can play a crucial role in reducing the risk of Alzheimer's disease.
Fatty acids explained1
DHA and EPA are a major omega-3 fatty acid predominantly found in fish oils. They are called essential fatty acids, meaning that the human body cannot produce them on its own, so they must come from dietary sources. Make sure not to confuse omega-3s (like DHA and EPA) with omega-6s. These are a different class of fatty acids typically found in vegetable oils and nuts. They are much more common in most diets, and can promote inflammation when consumed in excess.
DHA and EPA are particularly important because the molecules are building blocks for neurons. This means that maintaining healthy levels of DHA and EPA supports neuronal membrane integrity, promotes healthy synaptic activity, and mitigates inflammation within the brain. Long-term, these fatty acids have been shown to help preserve cognitive abilities and delay the onset of dementia1.
Clinical insights on Alzheimer’s prevention
A growing body of research points to a direct correlation between DHA and EPA intake and a reduction in the risk for Alzheimer's. Animal studies provide compelling evidence, showing that diets rich in DHA can significantly reduce the formation of amyloid plaques, which are closely linked to Alzheimer’s pathology1.
Furthermore, in human epidemiological research (research that investigates the distributions and determinants of health-related events in populations), increased consumption of DHA through dietary sources like fish has been associated with lower incidence rates of Alzheimer’s, suggesting its significant protective effect. One study3 found that people with the highest levels of DHA had a 49% lower risk of developing Alzheimer's disease compared to those with the lowest levels. This means that those in the top 20% were about half as likely to get Alzheimer's as those in the bottom 20%. Additionally, increasing DHA levels from the lowest group to the highest group was predicted to give an extra 4.7 years of life free from Alzheimer's disease.
Other studies have concluded similar results, showing a 47%5 reduction in risk, though there is debate about when this effect may occur. The consensus is that DHA supplementation is most effective when started early, before symptoms get classified as dementia6.
Increasing your omega-3 intake
There are two main ways to make sure you’re getting enough DHA and EPA - either making conscious dietary choices4 or taking supplements. From the diet side, fatty fish are an excellent source of omega-3s. Typical guidance recommends eating fish like salmon, mackerel, herring, or halibut at least 3 times per week. It’s worth noting that chia seeds and flax seeds are also excellent sources of omega-3s. Predatory fish like tuna are also good sources of EPA and DHA, but be careful not to consume them too often since they also contain high levels of mercury.
Fish oil supplements can be another great way to increase your intake of omega-3s - if you carry the APOE4 gene, supplementation is particularly important since you may have more trouble absorbing dietary omega-3s. However, it’s important to recognize that not all supplements were created equal. Specifically, not all brands will have the same purity of fatty acids, and not all will contain sufficient levels of DHA and EPA. Here are some things to look out for to make sure you are getting high quality fish oil:
- High amounts of DHA and EPA per serving (at least 500mg combined per serving)
- Minimal additives in the ingredients other than the oil and capsule contents
- Packaged in dark containers to protect the oil from light
A Step Towards Cognitive Longevity
Embracing a diet that includes adequate amounts of DHA and EPA can significantly contribute to brain health and potentially decrease the risk of Alzheimer’s. Start by evaluating your current dietary habits and consider how you might improve your omega-3 intake, ensuring your brain remains vibrant and healthy well into later life.
Where to get started
- Measure your blood omega-3 index to learn your current EPA and DHA levels. This is one of the 50+ biomarkers tested during your BetterBrain Essentials blood draw.
- Eat at least 3 servings of fatty fish (e.g., salmon, mackerel) per week, but make sure not to overdo your intake of predatory fish like tuna.
- Consider using fish oil supplements to increase your EPA and DHA intake. We recommend Carlson’s fish oil, which is available at a discount with a BetterBrain membership.

The Role of Homocysteine in Dementia Risk
Homocysteine is a naturally occurring amino acid in our body and can spike acutely, such as after staying up all night. In healthy people, homocysteine naturally clears over time. However, at chronic high concentrations, it is associated with various health issues, including heart disease and, notably, cognitive decline. In fact, having blood homocysteine levels over 14 μmol/L is associated with a nearly doubled risk of dementia1. Luckily, there are simple ways to lower your homocysteine levels - most notably B vitamin supplementation.
Brain Atrophy, Aging and Cognitive Decline
As we age, our brains naturally undergo some amount of atrophy, or decrease in size, which involves a loss of neurons and their connections. This process is accelerated in Alzheimer’s dementia2. With a lower brain volume and fewer neural connections, it’s easy to see how atrophy can lead to lasting cognitive impairment. One factor that has a strong influence on the rate of brain atrophy is blood concentration of homocysteine. Several studies3,4 link elevated homocysteine levels are linked with a heightened risk of dementia.
The role of B vitamins
You won’t often hear us say this, but you have an ace up your sleeve in fighting homocysteine: B vitamins. One study2 investigated the effects of using B6, B9, and B12 vitamins over the course of two years, using the same level of rigor that is commonly used for drug clinical trials.
On average, people who used B vitamins lowered their overall homocysteine levels by 32% and experienced a 30% slower rate of brain atrophy. In fact, those who started with very high levels of blood homocysteine (> 14 μmol/L) managed to slow their atrophy rate by 53%. In other words, this study suggests that the simple act of taking a daily B vitamin supplement can cut your dementia risk in half.
The type of B vitamin matters
There are two factors to consider when selecting a B vitamin supplement. The first is what vitamins you are getting. The study mentioned above specifically tested the use of vitamins B6, B9 (also known as folate), and B12. It’s important to get a mix of both. The second is whether or not you select the methylated form of the vitamins. Methylation is a biological process that makes the vitamins more available for your body to use. In other words, the same dose of methyl-B vitamins will be more strongly absorbed than normal B vitamins. This is especially important for people with mutations in the MTHFR gene, since they otherwise have trouble absorbing B vitamins. We generally recommend taking methylated B vitamins since they are perfectly safe, but if you are sensitive to overmethylation, you may want to consider regular B vitamins to avoid side effects like headaches, anxiety, or irritability.
Broader Implications for Dementia Prevention
Homocysteine is a critically important risk factor for dementia. Not only does it accelerate brain atrophy, it also aggravates other conditions through inflammation and oxidative stress. Thankfully, B vitamins are an extremely effective tool to lower homocysteine levels. While there are many other ways of managing your homocysteine levels, most notably through diet, exercise, and stress management, B vitamins are a low-effort high-impact way to keep your brain atrophy at bay.
Get started on managing your homocysteine
- Measure your blood homocysteine levels to learn where you stand. Homocysteine is one of the 50+ biomarkers tested during your BetterBrain Essentials blood draw.
- Consider using B vitamin supplements to lower your homocysteine, ideally below 9 μmol/L. We recommend Pure Encapsulations MethylAssist, but make sure you use an unmethylated alternative if you are sensitive to overmethylation.
- Learn more about homocysteine on the Peter Attia Drive episode on dementia. This episode covers many topics, so if you’re just interested in homocystine, skip ahead to 1:09:00.

Rapamycin: Revolutionizing Alzheimer's Prevention?
In the 1960s, researchers on Easter Island were investigating local indigenous peoples’ claims that the soil has healing properties. After testing various soil samples, the researchers isolated a small molecule they believed was responsible for the effects. They named it rapamycin5, after the traditional name for the island, Rapa Nui. Since its discovery, rapamycin has been used in various settings, from an antifungal agent to more recently a beacon of hope in anti-aging medicine. Additionally, it is showing promise in extending lifespan and preventing neurodegenerative diseases such as Alzheimer’s.
From anti-rejection med to longevity enhancer
The transition from an antifungal to a potential longevity drug has been intriguing. Rapamycin, approved in 1999 for its immunosuppressant qualities, is still commonly used in kidney transplants to prevent organ rejection. However, a 2014 study1 on older adults revealed a paradox: at much smaller doses, rapamycin boosted the immune response to flu vaccinations, despite their age-related weakened immune function. This unexpected enhancement suggests that rapamycin might have broader applications for disease prevention in older adults, potentially making it a valuable tool in combating age-related declines in the human immune system.
How rapa works
To understand how rapamycin works, it’s important to understand the molecule that it targets: a cellular receptor named mTOR. mTOR is present in nearly all cells in the human body and is responsible for mediating pathways that regulate cell growth, metabolism, and survival. Inhibiting mTOR completely is catastrophic - it prevents cells from making energy, eventually leading to their death. However, partial inhibition means that mTOR has a harder time forming a cluster with other proteins, which makes the cell act as if it's not getting enough food. This starts a process where the cell breaks down unneeded or damaged parts, like proteins that aren't folded correctly, which can otherwise impair the cell’s ability to function. This leads to improved cellular survival and resilience and is particularly relevant to brain health since one of the main features of Alzheimer’s is the accumulation of misfolded amyloid beta protein plaques in neurons.
The partial inhibition of mTOR therefore shows potential for slowing down the progression of Alzheimer’s disease and improving the survival rate of neurons. Animal studies2,3 suggest that rapamycin may help mitigate or improve many of the pathologies associated with Alzheimer's disease and potentially restore cognitive function.
Growing evidence yet limited human trials
While animal studies have robustly demonstrated lifespan and healthspan extensions—with remarkable outcomes like a 20-30% increase in the lifespan of mice4—human data remains scarce. The gap in human trials can be largely attributed to the fact that rapamycin use for longevity is considered “off-label”. This means that the Federal Drug Administration (FDA) has not yet approved rapamycin for this use, which diminishes incentives for comprehensive research funding. However, the evidence from animal studies across a variety of species strongly suggests a significant potential for rapamycin in anti-aging treatments.
Rapamycin’s mainstream use
As mentioned earlier, the FDA has only approved rapamycin for use as an immunosuppressant. It’s important to recognize that rapamycin use for longevity is still considered experimental and will not be reimbursed by insurance. Because the FDA hasn’t established guidelines around its use, there is no single accepted protocol for rapamycin dosage. Given the drug’s complex effects, the risk of experiencing side effects is real. Nonetheless,many individuals already use rapamycin “off-label” under the supervision of a physician for its longevity benefits. This is a perfectly legitimate use of the molecule, even though there is a lot we have yet to learn.
A promising option for the future
Rapamycin offers a compelling glimpse into the future of longevity and neuroprotection. Although its journey from a soil sample to a potential anti-aging miracle has been gradual, the promise it holds could change the landscape of preventive health. As research continues, both the medical community and potential users must weigh the benefits against the uncertainties of translating animal model successes to human health outcomes.
Learn more
Listen to the Peter Attia Drive episode on rapamycin to learn more about the molecule, its history, how it works, and the most recent evidence on its effects.

Dietary Defenders: Prebiotic Fibers in Alzheimer's Prevention
As Alzheimer's disease continues to impact millions globally, the scientific community is increasingly focusing on the gut-brain axis. This complex communication network, which links the gastrointestinal tract and the brain, could play a major role in preventing cognitive decline. Recent discoveries1 have shown that gut microbiota might affect everything from brain development to behavior to disease states, and researchers are starting to explore how the gut-brain axis can influence dementia risk.
Exploratory study: A closer look at fiber's impact on aging brains
The School of Life Course & Population Sciences at King’s College London spearheaded a pivotal double-blind study2 (the same type of study as used for clinical trials) with participants over 60 years old. Their research aimed to uncover the cognitive effects of consuming prebiotic fibers compared to a placebo.
Fiber fuels cognitive fortitude
Like any organism, the components making up the gut microbiome need food to survive. One source of nutrients for them is prebiotic fibers, such as inulin and fructooligosaccharides (FOS), both of which were the focus of the King’s College study. The researchers found that participants who took prebiotic supplements had more of one species of healthy bacteria called Bifidobacterium in their gut. This species has previously been linked to better cognitive performance, and indeed the participants who took supplements showed improved cognitive function scores through the same memory tests that are used as an early indicator of Alzheimer’s disease.
Why is this happening?
The composition of the gut microbiome has drastically changed over human history. Advances in agriculture, industrialization and globalization may have caused a decrease in gut microbial diversity, which has been associated with worse health outcomes. In particular, a review of multiple studies1 suggests that changes in the microbiome can lead to behavioral changes. In another study3 comparing 25 patients diagnosed with Alheimer’s disease to 25 healthy individuals, those with Alzheimer’s were found to have reduced gut microbial diversity.
Keeping an eye on your intake
Let’s get specific. Women should aim to consume 21-25g of fiber per day. Men should aim for 30-38g4. Here is a list of some common fiber-dense foods to consider adding into your diet.
A promising path to cognitive health
Emerging evidence connecting dietary habits, gut microbiota, and brain function highlights a novel approach to combat Alzheimer’s disease. The gut-brain axis is still a new area of research - there is much we don’t know, and many researchers around the world are investigating the different ways in which the microbiome influences our brain health. Such studies not only pave the way for innovative therapeutic avenues but also emphasize the profound impact our diet can have on mental and overall health.
Putting the science in action
- Eat enough fiber each day to make sure you are nourishing your gut microbiome. Women should strive for 21-25g daily, while men should aim for 30-38g.
- Learn more about the importance of your gut health on your brain and body through the Peter Attia Drive podcast.some text
- Episode #215 goes in-depth on the GI system - skip to 34:30 for ways in which the gut and brain communicate, and to 1:55:00 for ways to promote your gut microbiome using your nutrition.
- Episode #283 discusses the microbiome specifically - learn more about the importance of fiber at 38:30 and about the gut-brain axis at 50:15.
Get immediate insights with a 3 minute assessment
Start now.png)
GreyMatters
Grey Matters: June is Brain Awareness Month: a friendly reminder
A few reminders worth repeating
The fundamentals matter. Movement, sleep, nutrition, and social connection show up in the research again and again, and the earlier you start working on them, the more they compound.
But the fundamentals are just the starting point. Brain health is also deeply individual, and what moves the needle most for one person may not be what moves it for you. Depending on your biology, your genetics, your biomarkers, and your specific risk factors, the right plan might involve targeted supplementation, hormone or metabolic interventions, cardiovascular work, cognitive training, or addressing things like sleep apnea or inflammation. That's exactly why knowing your baseline matters so much. It turns a generic checklist into a plan built around you.
What our members are saying
"I put off getting tested for years because I figured there was nothing I could do. BetterBrain showed me exactly where I stood and gave me a plan. I wish I'd started sooner." — John O.
"Having a coach who actually checks in made all the difference. I've never been this consistent with my health." — Caroline T.
"Knowing my numbers took away the fear. Now it just feels like something I'm in control of." — Sandra W.
Consider this your friendly nudge
If brain health has been on your mind, this is a good month to act on it. Getting started is simple, much of it may be covered by insurance, and your future self will thank you.
And if you've already started on your BetterBrian journey consider forwarding this to a friend to help them take that next step.
Share this referral link and they'll get Essentials labs (50+ biomarkers) for just $39 (normally $89), plus access to $0 coaching with insurance.
Grey Matters: See the research behind every recommendation
Hey there,
There's a lot of brain health advice on the internet, and most of it comes with the same problem: no way to tell where it came from or if it's trustworthy. Someone tells you sauna is good for your brain, or that you should be lifting, or that omega-3s matter, and you're left to either take it on faith or go digging through PubMed yourself. Most people, reasonably, just take it on faith.
We've never loved that, because trust in health advice should be earned, not assumed. So we did two things worth telling you about.
The Content Library
First, if you haven't spent time in the Content Library inside your dashboard, it's worth a look. It's a growing, curated collection of the best brain health content we can find: videos, podcasts, articles, and clips, pulled from people who actually know what they're talking about. Think Andrew Huberman on light and sleep, Rhonda Patrick on sauna and exercise, our own CSO Tommy Wood on reducing cognitive decline, and a lot more.
You can search it, filter by format, and save what you want to come back to. And BeBe can point you to the right thing for wherever you are: if you ask about sleep, it can hand you the specific episode worth your time instead of making you wade through everything. It's the difference between a search engine and a good friend who's already done the reading. If you're not a BetterBrain client yet, you can access the Content Library for free with a Self-Directed account.
Technique Spotlight
The studies behind your plan
This is the part we're most excited about. Every technique and recommendation in your BetterBrain plan is now linked to the actual research behind it, the specific studies connected to the specific practice, biomarker, or system they support. When BeBe or your coach suggests something, you can trace it straight to the evidence and see how strong it is.
This was a big project and it brings roughly 1,500 studies into the app, mapped to the techniques and markers they relate to. Weak or unsupported studies were deliberately left out, so what's linked is the evidence we'd actually stand behind.
Here's why that matters. Not every recommendation carries the same weight. Some are backed by large randomized trials, others by smaller or observational work, and you deserve to know which is which. Linking the studies keeps us accountable to the evidence and lets you make informed decisions instead of just following instructions. It's the same standard we hold ourselves to internally: when a new study comes out, we read it, assess it, and only fold it into what we recommend if it holds up.
How this relates to brain health
Brain health is a field with real science and a lot of noise, and the two are easy to confuse. We try to stay on the science side of that line and be honest about what's solid, what's promising, and what's still an open question. Making the research visible is that principle made concrete. If we recommend it, you should be able to check it.
If you want to explore, open a technique and scroll to the bottom to see the relevant studies or ask BeBe why it recommends any technique in your plan, and follow the research yourself.
And if you're reading this as someone who hasn't started with us yet: this is what BetterBrain is, evidence-based brain health guidance you can verify, not wellness advice you have to trust blindly. BetterBrain coaching is covered at $0 for 92% of approved clients. See if you're covered.
Know someone who might benefit from BetterBrain?
Share this referral link and they'll get Essentials labs (50+ biomarkers) for just $39 (normally $89), plus access to $0 coaching with insurance.
An 11-country trial tested brain health advice against structured support
The same brain health advice produced very different results
Most people already know the broad advice for protecting their brain. Exercise regularly. Eat well. Manage blood pressure and blood sugar. Stay socially and mentally engaged. Get enough sleep.
The harder part is following through consistently, especially when work gets busy, routines change, motivation fades, or the original plan does not fit your life very well.
A two-year randomized trial across eleven Latin American countries has now put a number on how much that harder part is worth. Both groups worked on the same broad areas of brain health. One group received ongoing coaching, supervision, and regular group meetings. The other received health education and general recommendations. After two years, the structured group showed 55 percent greater improvement in overall memory, thinking, and reasoning.
The trial, called LatAm-FINGERS, was published in The Lancet and presented at the Alzheimer's Association International Conference.
What the trial tested
The study included 1,065 older adults who were at elevated risk of cognitive decline but did not have dementia. It ran across twelve sites in eleven countries and followed participants for two years.
Both groups worked on the same broad areas of brain health, including physical activity, nutrition, cognitive training, social engagement, and management of cardiovascular risk. The difference was the amount of structure surrounding the work.
The flexible group, 526 participants, attended four meetings over two years. They received health education and general recommendations, but no ongoing coaching or supervision.
The structured group, 539 participants, received supervised exercise, nutrition counseling, cognitive training, cardiovascular risk monitoring, ongoing coaching, and 38 group meetings that provided social connection and accountability.
In other words, the trial was not testing whether lifestyle matters for the brain. That question has been asked before. It was testing how much the way a program is delivered can change the results it produces.
What happened
After two years, the structured group showed 55 percent greater improvement in overall memory, thinking, and reasoning than the more flexible group. They also had greater improvements in executive function and processing speed.
Both groups were working on their brain health, and both improved. The structured group simply improved much more.
That makes the finding more interesting than a comparison between doing something and doing nothing. The broad recommendations were similar. What changed was the frequency of contact, the level of supervision, and the support participants received while putting those recommendations into practice.
Because participants were randomly assigned to the two groups, differences in motivation or baseline health are less likely to explain the result. The structured program itself appears to have contributed to the additional cognitive improvement.
Heather Snyder of the Alzheimer's Association, commenting on the results at the conference, put it simply: "A key message from this study is that structure and social support matter."
The finding builds on the original FINGER trial in Finland, which found that a multidomain lifestyle program could help protect cognitive function in older adults at risk of decline. LatAm-FINGERS took that model and adapted it to local cultures, diets, and habits rather than importing it unchanged, which matters for anyone wondering whether these programs travel.
Read the full LatAm-FINGERS study
What structured support actually does
A brain health plan can look simple on paper and still be difficult to carry out.
A person may leave an appointment intending to exercise four times a week, improve their sleep, change their diet, take several supplements, and reduce stress. Every recommendation may be reasonable. The problem is that seven reasonable priorities are still seven priorities competing with the rest of life.
A few weeks later, the easiest habits are sometimes still happening. The more inconvenient ones have started to disappear, which is where structured support comes into play. It creates a regular opportunity to review what happened, understand why something did not work, and adjust the action plan before one missed week becomes a habit that has quietly been abandoned.
Sometimes the person needs accountability. Sometimes the goal was too ambitious. Sometimes the recommendation needs to change because of travel, an injury, family responsibilities, or a demanding period at work.
The goal is not to follow the original plan perfectly. It is to keep adjusting the plan until it works in real life.
The question the study leaves open
LatAm-FINGERS compared a structured, intensive program with a more flexible, self-guided version focused on the same broad areas of brain health. It did not test whether a personalized action plan works better than a generic one. That is a separate question, and an important one.
Two people can receive the same list of brain health recommendations and have very different needs. One person may need to focus on blood pressure. Another may need to address poor sleep, low cardiovascular fitness, insulin resistance, or a nutritional deficiency first. The markers that shape brain health sit across sleep, metabolic health, cardiovascular health, inflammation, and nutrition, and they do not line up the same way in any two people.
A useful brain health system needs to answer two questions. What matters most for this person, and what will help them keep doing it?
Personalization helps determine the priorities. Structure helps turn those priorities into sustained action.
How BetterBrain approaches both
BetterBrain is one connected system that brings together brain-relevant health information, a personalized action plan, and continued support.
There are two ways to start.
Some people begin with Blueprint, which uses more than 50 brain-relevant biomarkers, cognitive testing, health history, and lifestyle information to identify the areas that matter most for their brain health, with a nurse coach to walk through what the results mean. Instead of receiving a broad list of everything they could improve, they get a personalized action plan ranked by impact.
Others begin with the Coaching Program, where a dedicated brain health coach helps build the action plan, checks in on progress, and adjusts it when life gets in the way. Coaching is often fully covered by insurance, and many commercially insured clients pay nothing out of pocket.
Both starting points lead toward the same goal: a smaller set of meaningful priorities, a realistic action plan, and enough continued support for that plan to last.
The bottom line
The LatAm-FINGERS trial moves the brain health conversation beyond whether lifestyle matters. It shows that the way lifestyle guidance is delivered can meaningfully change the outcome.
Advice alone leaves people responsible for setting priorities, creating a schedule, tracking progress, solving barriers, and knowing when to adjust the plan. A better delivery system does those things with them. It provides clear priorities, regular contact, accountability, opportunities to review progress, and a way to adapt when the original plan stops working. That support helps healthy actions continue long enough to produce meaningful results.
Personalization helps you choose the right actions. Structure helps you keep doing them.
How to Keep Your Brain Sharp at Any Age: 6 Lessons From Dr. Tommy Wood on Huberman Lab
Our Chief Science Officer, Dr. Tommy Wood, joined Andrew Huberman on the Huberman Lab podcast for a nearly three-hour conversation titled "Accelerate Learning & Increase Cognitive Capacity." His core message: your brain keeps adapting to whatever you ask of it, at 40 and at 75. Staying sharp is less about your age and more about whether you keep giving your brain new, challenging inputs, move your body before and around mental work, eat a high-quality overall diet, and test your biomarkers instead of guessing at supplements.
Here are the six takeaways we think are most worth acting on, plus where to start if you want to put them into practice.
Does aging itself cause cognitive decline?
Not in the way most people assume. According to Wood, aging itself is not the primary driver of decline. Your brain keeps the capacities you use and prunes the ones you stop using, so much of what we call age-related decline comes from no longer giving the brain new, challenging inputs. Encouragingly, he notes that mental processing speed tends to hold steady until around age 60.
That reframing matters. If decline is largely about disuse rather than age, then the inputs you choose, at any age, are levers you control.
What activities actually keep your brain sharp?
The activities that build cognitive capacity share three traits: they are new, hard, and ideally social.
Crosswords and sudoku, Wood points out, are more relaxing than challenging. They exercise skills you already have. To actually build capacity, pick something that stretches you and mixes movement, thinking, and other people:
- Dancing has the best evidence, ballroom and square dancing especially
- Ball sports and martial arts
- Learning a language
Part of the trick is getting comfortable being a beginner. The discomfort of making mistakes is not a sign you picked the wrong activity. It is what drives the learning.
Do you need to be in a flow state to learn?
No. Real learning, and even peak performance, often happens in what athletes call a clutch state, where the work still feels like hard work.
What matters more is structure. Hard mental work is really only sustainable in 20 to 30 minute focused blocks, so work in chunks and protect them from distraction. Even having a phone in the room carries a cost to focus.
How does exercise improve learning and memory?
Wood describes exercise as two brain tools in one:
- In the moment: a short 20 to 30 minute jog or strength session right before mental work sharpens learning during that session.
- Over time: harder aerobic work, like intervals, builds the hippocampus and supports memory, while resistance training builds the brain's white matter and supports decision-making.
The practical answer to "cardio or weights for brain health?" is both, and if you can, schedule some of it right before your most demanding mental work.
What should you eat, and should you take supplements?
On diet, whole-food patterns like the Mediterranean and MIND diets have the best evidence, and it is overall diet quality, not any single food, that matters.
On supplements, Wood's advice is to test your levels rather than guess, because the standard "normal" lab range is not the same as the optimal one. His clearest example: omega-3 and B vitamins only work when you have both. That interdependence is exactly why we measure homocysteine and other brain-specific biomarkers in Blueprint rather than blanket-recommending a supplement stack.
For supplements with modest, real support, he points to creatine and a basic omega-3 plus B-vitamin stack. Our picks in those categories, including Advanced DHA, Thorne Creatine, and MethylAssist, are all in the Picks library, and Picks is now HSA/FSA eligible through our partnership with TrueMed.
What else protects long-term brain health?
Some of the biggest protections are indirect. Blood pressure, cholesterol, hearing, and metabolic health all shape long-term brain health. Avoiding serious illness matters too, because cognition tends to step down after a major sickness rather than declining smoothly.
One finding Wood flags as worth watching: the shingles vaccine has been associated with lower dementia risk across several large studies.
Where to start
You do not need a perfect routine or new technology. The conversation points to a short list: work on something hard and a little new, move before mental work, get real sleep, and test before you supplement.
That last step is where BetterBrain can help. Blueprint covers the testing, 50+ biomarkers plus cognitive testing and a 1:1 consultation to walk through your results, for $89 with insurance. And if you finish your results thinking "okay, but what should I actually do," that is what our 12-week Coaching Program is for. 92% of eligible customers pay $0 with insurance.
If you want to go deeper, listen to the full episode, and check out Tommy's new book, The Stimulated Mind: Future-Proof Your Brain from Dementia and Stay Sharp at Any Age, which covers the same ground in more depth through his 3-S model: challenge the brain, feed it, and let it recover.
Frequently asked questions
At what age does cognitive decline start?
Later than most people think. Wood notes that mental processing speed tends to hold steady until around age 60, and that much of what we attribute to aging actually reflects reduced challenge. The brain keeps what you use and prunes what you stop using, at any age.
Are crosswords and sudoku enough to keep your brain sharp?
Probably not. Wood describes them as more relaxing than challenging, since they exercise skills you already have. To build new capacity, choose activities that are new, hard, and social, like dancing, ball sports, martial arts, or learning a language.
What is the best exercise for brain health?
Both aerobic and resistance training, for different reasons. Harder aerobic work like intervals builds the hippocampus and supports memory, while resistance training builds white matter and supports decision-making. A 20 to 30 minute session right before mental work also sharpens learning in the moment.
Should I take supplements for brain health?
Test first. Standard "normal" lab ranges are not the same as optimal ranges, and some nutrients depend on each other. Omega-3 and B vitamins, for example, only work when you have both, which is why measuring biomarkers like homocysteine beats guessing. Creatine and a basic omega-3 plus B-vitamin stack have modest, real evidence behind them.
You Can Now See the Studies Behind Every BetterBrain Recommendation
There's a lot of brain health advice on the internet, and most of it comes with the same problem: no way to tell where it came from or whether it's trustworthy.
Someone tells you sauna is good for your brain. Or that you should be lifting. Or that omega-3s matter. And you're left to either take it on faith or go digging through PubMed yourself. Most people, reasonably, just take it on faith.
We've never loved that. Trust in health advice should be earned, not assumed. So we did two things worth telling you about.
The Content Library: curated, not crowdsourced
If you haven't spent time in the Content Library inside your dashboard, it's worth a look. It's a growing, curated collection of the best brain health content we can find: videos, podcasts, articles, and clips from people who actually know what they're talking about.
Think Andrew Huberman on light and sleep. Rhonda Patrick on sauna and exercise. Our own Chief Science Officer, Dr. Tommy Wood, on reducing cognitive decline. And a lot more.
You can search it, filter by format, and save what you want to come back to. And BeBe, our AI assistant, can point you to the right thing for wherever you are. Ask about sleep, and it hands you the specific episode worth your time instead of making you wade through everything. It's the difference between a search engine and a good friend who's already done the reading.
Not a BetterBrain client yet? You can access the Content Library for free with a Self-Directed account.
The studies behind your plan
This is the part we're most excited about.
Every technique and recommendation in your BetterBrain plan is now linked to the actual research behind it: the specific studies connected to the specific practice, biomarker, or body system they support. When BeBe or your coach suggests something, you can trace it straight to the evidence and see how strong it is.
This was a big project. It brings roughly 1,500 studies into the app, each mapped to the techniques and markers it relates to. Weak or unsupported studies were deliberately left out, so what's linked is the evidence we'd actually stand behind.
Why evidence strength matters
Not every recommendation carries the same weight. Some are backed by large randomized controlled trials. Others rest on smaller or observational work. You deserve to know which is which.
Linking the studies does two things. It keeps us accountable to the evidence. And it lets you make informed decisions instead of just following instructions.
It's the same standard we hold ourselves to internally: when a new study comes out, we read it, assess it, and only fold it into what we recommend if it holds up.
Why this fits how we think about brain health
Brain health is a field with real science and a lot of noise, and the two are easy to confuse. We try to stay on the science side of that line and be honest about what's solid, what's promising, and what's still an open question.
Making the research visible is that principle made concrete. If we recommend it, you should be able to check it.
How to explore
Open any technique in your plan and scroll to the bottom to see the relevant studies. Or ask BeBe why it recommends any technique in your plan, and follow the research yourself.
And if you're reading this as someone who hasn't started with us yet: this is what BetterBrain is. Evidence-based guidance to sharpen your brain health now and reduce dementia risk long-term, backed by research you can verify rather than wellness advice you have to trust blindly. BetterBrain coaching is covered at $0 for 92% of approved clients. See if you're covered.
Bottom line
The Content Library puts the best brain health content in one curated place. And every technique in your plan is now linked to the real research behind it.
Trust in health advice should be earned. Now you can check ours.
How Chronic Stress Shrinks Your Brain, and How to Reverse It
Chronic stress does more than affect your mood. Sustained cortisol exposure physically shrinks the hippocampus, your brain's primary memory center. The encouraging part: this is reversible. In controlled neuroimaging studies, eight weeks of mindfulness practice increased gray matter in the hippocampus and reduced it in the amygdala, the brain's threat-detection center. Managing stress is one of the most accessible ways to protect your long-term cognitive health.
Stress is easy to file under "quality of life" rather than "brain health." The neuroscience tells a different story, and it's a hopeful one, because the same biology that makes chronic stress harmful also makes it one of the most modifiable risks you can act on.
Below, we cover what chronic stress does to the brain, the landmark study showing mindfulness can reverse it, the techniques that actually work, and how to measure your progress.
What does chronic stress do to your brain?
When your brain perceives a threat, it releases cortisol. In short bursts, this is helpful, it sharpens your response to a genuine challenge. The problem is sustained elevation.
Under chronic stress, prolonged cortisol exposure becomes toxic to neurons, and the hippocampus is especially vulnerable because it is packed with cortisol receptors. Over time, that exposure causes the neural branches that let brain cells communicate to shrink. The downstream effects are measurable: reduced hippocampal volume, fewer new brain cells, and impaired memory.
This matters beyond day-to-day forgetfulness. Hippocampal shrinkage is one of the earliest detectable structural changes in Alzheimer's progression, and chronic psychological stress is now recognized as a modifiable dementia risk factor in its own right. In other words, stress sits on the same biological pathway as accelerated cognitive aging, which is precisely why acting on it has such a high return.
Can mindfulness reverse stress-related brain changes?
Yes, and the evidence comes from before-and-after brain imaging, not self-report.
In 2011, researchers at Harvard-affiliated Massachusetts General Hospital published a landmark neuroimaging study. Using MRI, they measured gray matter density in healthy adults before and after eight weeks of mindfulness practice. Participants showed measurable increases in gray matter in the hippocampus and in regions involved in learning and emotional regulation. At the same time, gray matter in the amygdala, the brain's primary stress and threat-detection center, decreased. A control group who did not practice mindfulness showed none of these changes.
The design is what makes it compelling. This was not a comparison of lifelong meditators against non-meditators, where genetics or lifestyle could explain the difference. It was imaging of the same brains, across just eight weeks of practice. You can read the full study here.
How does stress management protect the brain?
Mindfulness and related practices work through a few overlapping mechanisms. They reduce cortisol output, calm the amygdala's threat response, and lower the chronic, low-grade inflammation associated with sustained stress. These are the same pathways implicated in accelerated cognitive aging, so quieting them protects the brain on more than one front at once.
The practical implication is freeing: you do not need the "perfect" technique. You need to move these levers consistently, and there is more than one way to do that.
What stress management techniques actually work?
Different techniques reach the same biology through different doors, which means you have options. These are the Essential, evidence-based interventions to start with:
- Slow, deep breathing. Controlled breathing activates your parasympathetic nervous system, your body's "rest and digest" mode. Even a few minutes measurably reduces cortisol and heart rate. For many people this is the easiest entry point.
- Mindfulness meditation. The technique behind the brain-imaging study above. Consistent practice, even 8 to 10 minutes daily, produces measurable effects on stress hormones and self-reported stress within a few weeks.
- Nature exposure. Time in natural environments is associated with lower cortisol, lower blood pressure, and improved mood. The effect appears to be dose-dependent, so more time outdoors tends to help more.
- Social support. Strong social connections help buffer the brain against the effects of stress.
How do you start a 10-minute mindfulness practice?
You do not need a cushion, an app, or a quiet mind. Here is the whole practice:
Find a quiet spot and sit comfortably. Bring your attention to the physical sensation of your breath, the air moving in and out. Your mind will wander. That is not failure, that is the exercise. Each time you notice it drifting and bring it back, you are doing the rep that builds the skill. There is no perfect posture and no requirement to empty your mind. Just ten minutes of practicing the return.
A note on getting started: Don't overthink which technique to begin with. If sitting meditation feels like a stretch, start with a few minutes of slow breathing or a walk outside. The research is clear on this point: the technique that protects your brain is the one you will actually do.
How can you track stress and its effects on the brain?
You can't feel your inflammation dropping, but you can measure it. Chronic stress shows up in bloodwork as elevated hs-CRP, one of the same inflammatory markers associated with cognitive decline. When a stress-management practice starts working, that number moves, and lab panels let you watch it happen.
The effects ripple outward from there. Sleep quality typically improves within weeks of consistent practice, and better sleep gives your glymphatic system, your brain's overnight waste-clearance crew, more time to do its job.
This is what makes stress management such a high-leverage intervention. It rarely works alone. Better stress regulation improves your sleep, better sleep amplifies the benefits of exercise, and lower inflammation makes anti-inflammatory nutrition work harder. Pull one lever, and the whole system responds.
The bottom line
Chronic stress physically changes the structure of your brain, and mindfulness and related practices can measurably change it back. You don't need to overhaul your life to benefit. Ten minutes of breathing or meditation, a walk outside, or time with people you care about all move the same biology. Start with whatever feels easiest, stay consistent, and let the results compound.
If you're working with a Brain Health Coach, the De-Stress section of your protocol is a natural starting point.
Ready to build a personalized stress management practice? Check if your insurance covers coaching.
Frequently asked questions
Does stress really shrink your brain?Yes. Sustained cortisol exposure from chronic stress is associated with reduced hippocampal volume, the brain region responsible for memory. It also reduces the formation of new brain cells and impairs memory over time.
Can you reverse brain changes caused by stress?Evidence suggests you can. In a 2011 MRI study, eight weeks of mindfulness practice increased gray matter in the hippocampus and decreased it in the amygdala in the same participants, changes not seen in a non-practicing control group.
How long does it take for mindfulness to change the brain?Structural changes were measurable after eight weeks of practice in controlled imaging studies, and effects on stress hormones and self-reported stress often appear within a few weeks.
What is the best stress management technique for brain health?There is no single best technique. Slow breathing, mindfulness meditation, nature exposure, and strong social connection all work through overlapping pathways. The most effective one is the one you will do consistently.
Is chronic stress a risk factor for dementia?Chronic psychological stress is now recognized as a modifiable dementia risk factor. Hippocampal shrinkage, which stress contributes to, is one of the earliest structural changes seen in Alzheimer's progression.