GreyMatters
Educational articles, BetterBrain resources, latest in brain health, and news about us. Written for you, with expertise (and love).
VERVE-102: A One-Time Gene Edit for Cholesterol, and Why It's a Brain Story | BetterBrain
Every so often a piece of research comes along that makes you stop and appreciate how far medicine has come. This is one of those.
Researchers just reported early results for a one-time treatment that durably lowers LDL cholesterol by editing a single gene. One infusion, with effects that have held for up to a year and a half so far, and likely to last a lifetime. It's very early research in a small, specific group of patients, and it's years from a doctor's office. But the underlying biology is some of the most well-studied in all of cardiovascular medicine, and it connects directly to your brain.
Editing one gene to lower cholesterol
The therapy, called VERVE-102, targets a gene called PCSK9. PCSK9 is a protein that reduces your liver's ability to clear LDL cholesterol from your blood. The more PCSK9 activity you have, the fewer LDL "receptors" your liver keeps available to pull LDL particles out of circulation.
Here's the reassuring part: some people are born with naturally low-functioning PCSK9 genes, and they tend to have markedly lower LDL across their entire lives, substantially lower rates of heart disease, and no apparent downside. Turning down PCSK9 is a protective pattern scientists have studied for two decades. We already have approved PCSK9-lowering drugs; they just require ongoing injections.
What's new is the delivery. VERVE-102 uses base editing, a precise form of gene editing, to make a single change to the PCSK9 gene in liver cells after one infusion, doing once, durably, what current drugs do repeatedly. In the Heart-2 trial, a single dose lowered LDL by an average of around 50%, and by as much as roughly 69% at the higher doses, with reductions holding for up to 18 months and no treatment-related serious adverse events reported.
The honest caveats
The headline is easy to over-read, so here's the careful version. It's a phase 1b trial, an early stage focused on safety and initial signals in a small number of participants, and it has not been shown to prevent heart attacks, strokes, or cognitive decline. It enrolled a specific, high-risk group (inherited very high cholesterol or early coronary artery disease), so these are not general-population results. And gene editing is genuinely new: the PCSK9 mechanism is exceptionally well understood, but a permanent edit to a gene is a young field whose long-term safety story takes years to write. The likely path is approval first for very high-risk individuals, at significant cost, after a larger phase 2 trial.
Why this is a brain-health story
At BetterBrain, we look at the whole body, because your brain doesn't exist in isolation from it, and few things connect the two as directly as lipids.
Start with ApoB. You've probably heard of LDL cholesterol; ApoB is the more precise number underneath it. Every LDL particle carries exactly one ApoB protein, so LDL-C tells you the amount of cholesterol in LDL particles, while ApoB tells you the number of particles actually driving damage in your artery walls. When the two disagree, ApoB is the better predictor of risk. Lowering PCSK9, through these new therapies or the drugs we already have, lowers both.
Now connect it to the brain. The blood vessels that feed your brain face the same lipid-driven damage as the ones feeding your heart, and that vascular damage is one of the major pathways of cognitive decline. Protecting your lipids over a lifetime is protecting your brain, especially for people who tend to run higher LDL, including APOE4 carriers. That's one reason lipid management is a core part of what we do.
What this means for you, right now
You don't have to wait for a therapy that's years away. The target itself, your lipid health, is something you can measure and move today.
Get your ApoB tested, not just standard cholesterol, because it counts the particles actually driving damage. Think of lipids as a lifelong number: it's the decades of cumulative exposure that drive risk, so small, steady improvements compound in your favor, and starting earlier beats starting perfectly. Use the levers you already have, including diet, regular movement, and, where your physician recommends them, proven medications.
If you'd like to see where you stand, BetterBrain Blueprint covers ApoB and 50+ other markers and starts at $89 with insurance, and a BetterBrain coach can pull your full lipid picture into one clear plan, so that whatever arrives in five or ten years, you've protected the decades in between.

The Glymphatic System: Why Deep Sleep Is Your Brain's Best Cleanup Tool
What if the most important thing you could do for your brain tonight was also the most straightforward? Not a new supplement or a complicated protocol. Just better sleep, specifically the deep stages most people shortchange without knowing it.
Here is the biology that makes that matter more than most people appreciate.
Your brain has its own plumbing. It only fully runs at night.
Every other tissue in your body has a lymphatic system to carry away metabolic waste. For a long time, the brain was thought to be the exception, with no obvious mechanism for the job. That changed in 2013 when researchers described the glymphatic system: a network that uses cerebrospinal fluid to flush waste out of brain tissue, including amyloid-beta and tau, the proteins that accumulate in Alzheimer's disease.
The connection to sleep came alongside it. Glymphatic clearance is not constant. It ramps up dramatically during deep, slow-wave sleep, when the spaces between brain cells expand and fluid can move through more freely. This is one of the clearest biological explanations for why sleep is not optional maintenance. It is when a specific, measurable cleanup process actually runs, protecting your brain now and building resilience for decades to come.
What the newer research tells us about the engine
The system's existence has been well established for over a decade. What researchers kept working on was the mechanics: what physically moves the fluid?
A 2025 study published in Cell from Maiken Nedergaard's lab (one of the teams behind the original glymphatic work) helps answer that. In mice, the team found that during deep sleep a small brainstem region called the locus coeruleus releases norepinephrine in slow, rhythmic waves, roughly one every fifty seconds. Each wave gently tightens and relaxes the blood vessels, and that slow oscillation appears to drive cerebrospinal fluid through the brain, moving waste along.
The result connects three things already known to be related (deep sleep, blood-vessel tone, and fluid clearance) into a single mechanism. Deep sleep is not the brain idling. It is the brain running a coordinated pump.
Two points of context worth holding on to. First, this is animal research. The mechanism has been demonstrated in mice, whose sleep biology is a strong but imperfect model for humans. It tells us how the system likely works, not the conclusion of a human clinical trial.
Second, the same study found that zolpidem (the active ingredient in Ambien) suppressed these norepinephrine waves in mice and reduced fluid flow. That is a genuinely interesting signal, but it is a finding in animals about a mechanism, not evidence that a prescription harms people. If you take a sleep aid, this is not a reason to stop. It is a reason to make sleep quality a real conversation with your prescriber.
What this means in practice
None of this requires a new gadget. It gives you a sharper reason to take the fundamentals seriously.
Protect the deep-sleep window. Slow-wave sleep is concentrated in the first half of the night. A consistent wake time, morning light exposure within thirty minutes of getting up, and a cool, dark room are the most reliable ways to support it. These are habits that compound over years.
Be honest about alcohol and late meals. Both fragment the deep-sleep stages where clearance is most active. You may fall asleep quickly and still miss the part of the night that matters most for this system.
Treat sleep as something measurable. The same way we use biomarkers to track what is working, sleep consistency and quality are worth paying attention to over time rather than estimating from how you feel in the morning.
Take loud snoring or daytime exhaustion seriously. Both can signal sleep apnea, which repeatedly disrupts the deep sleep this system depends on. It is common, often undiagnosed, and very treatable.
If you use a sleep medication, bring the goal of better sleep quality to your prescriber rather than changing anything on your own.
BetterBrain's brain health coaches work with clients to turn sleep from a vague intention into a specific, trackable practice built around your schedule, your biology, and your data. Think sharper now, and protect your brain for decades.

Tommy Wood's 3-S Model: The Science Behind Future-Proofing Your Brain
The Framework Behind What We Do at BetterBrain
Our Chief Science Officer Tommy Wood published The Stimulated Mind in March 2026, and we think it's the most complete, accessible guide to dementia prevention that exists right now. A rigorous, science-backed model for understanding what your brain actually needs across a lifetime, written by someone who has spent his career studying exactly this.
At the center of the book is what Tommy calls the 3-S Model: Stimulation, Support (sleep and recovery), and Supply (of energy and nutrients). These aren't three separate suggestions. They're three categories of input the brain depends on, and Tommy's argument is that they reinforce each other in ways most people don't appreciate. They synergize, providing outsized benefits from even simple changes across all three.
BetterBrain is built around exactly this model. The 10 health systems and 11 practices our coaches work through with you are the operational version of what Tommy lays out in the book. Here's a breakdown of each S and one thing you can act on this week.
S1: Stimulation
The first S is the one that surprises people. Tommy's argument is that the brain, like muscle, needs ongoing challenges to maintain its structure. The variable that matters is novelty. Doing the same crossword every day is not stimulation in the sense your brain cares about. Learning a language, picking up a new instrument, or taking a class on something you have no prior context for, are stimulating.
This connects to what researchers call cognitive reserve: the buffer your brain builds through years of varied learning. Cognitive reserve is one of the strongest predictors of who maintains function in their 70s and 80s, even in the presence of pathology like amyloid plaques.
What you can do this week: Pick one thing this month that you don't already know how to do. It doesn't have to be heavy, a new recipe technique, a new fitness class, a new route on your morning walk that requires you to navigate. The brain treats novelty as a signal that it needs to keep adapting.
S2: Support (Sleep and Recovery)
The second S is the one most people know is important and still underestimate. Recovery, especially during sleep, is when the brain adapts and improves.
While you sleep, your brain runs a waste-clearance system that flushes out the proteins that build up during the day, including amyloid, the same protein that accumulates in Alzheimer's disease. Think of it like a dishwasher that only runs at night. Skip enough nights, or get consistently shallow sleep, and the dishes pile up. Disrupted sleep is associated with elevated pTau-217, lower cognitive scores, and higher long-term dementia risk.
Tommy is direct about this in the book: there is no supplement protocol that compensates for chronically poor sleep. And the work has to start with the structure of your sleep itself, meaning how much time you actually spend in the deep and REM stages, not just how many hours you're in bed. You can sleep eight hours and still miss most of the stages where the real restoration happens.
What you can do this week: Protect a consistent wake time. The wake time matters more than the bedtime because it anchors your body's internal clock. Pair it with morning light within 30 minutes of getting up, and you've done more for your sleep quality than most people manage with supplements or sleep trackers alone.
S3: Supply (Energy and Nutrients)
The third S is where a meaningful part of your biomarker picture lives. Your brain runs on a continuous supply of glucose, oxygen, omega-3 fatty acids, B vitamins, and a long list of micronutrients. Deficits in any of these can quietly compromise function for years before they show up as symptoms. When these markers are at optimal levels, they actively protect your brain, often for decades.
The first place to look is diet. What you eat every day is the primary driver of whether your brain gets what it needs. Targeted supplementation comes second, once you know where the gaps actually are.
The biomarkers we look at first in the Blueprint panel are homocysteine, vitamin D, vitamin B12, ferritin, and folate. These are the ones most likely to flag a nutrient supply problem before you feel it. And the fix is usually targeted, not maximal. Most clients don't need fifteen supplements, they need the right two or three, chosen based on what their labs actually show.
What you can do this week: If you haven't had a full brain-health panel in the past year, that's where to start. A nutrient gap rarely shows up in isolation, and the right intervention depends on seeing how everything fits together.
Why All Three Matter Together
The argument the book makes is that the components that support brain health aren't a long list of individual variables, they're an integrated network.
Stimulation without sleep doesn't give the brain time to consolidate. Sleep without nutrient supply leaves the brain trying to do its overnight work without raw materials. Nutrient supply without stimulation gives the brain everything it needs to grow but no reason to.
This is consistent with what BetterBrain's coaches see in practice. Clients who work hard on one of the three but ignore the others tend to plateau. The ones who address all three see the biggest shifts in biomarkers, cognitive scores, and how they actually feel.
The Bottom Line
The Stimulated Mind is the best communication of modern brain science available today, worth reading whether you're at the beginning of thinking about brain health or several years into a protocol.
Working with a BetterBrain coach to address all three Ss, across all 11 practices, is how you turn a framework into measurable results.
hs-CRP: The Biomarker Most Likely to Flag Silent Inflammation in Brain Health
If you have ever had a routine blood panel, you have probably seen "CRP" on the list. What you may not have seen is "hs-CRP," which sounds like the same test but is not. The difference matters a lot for brain health.
This piece walks through what hs-CRP measures, why it shows up in almost every BetterBrain protocol, and what to do if yours is elevated.
What hs-CRP measures
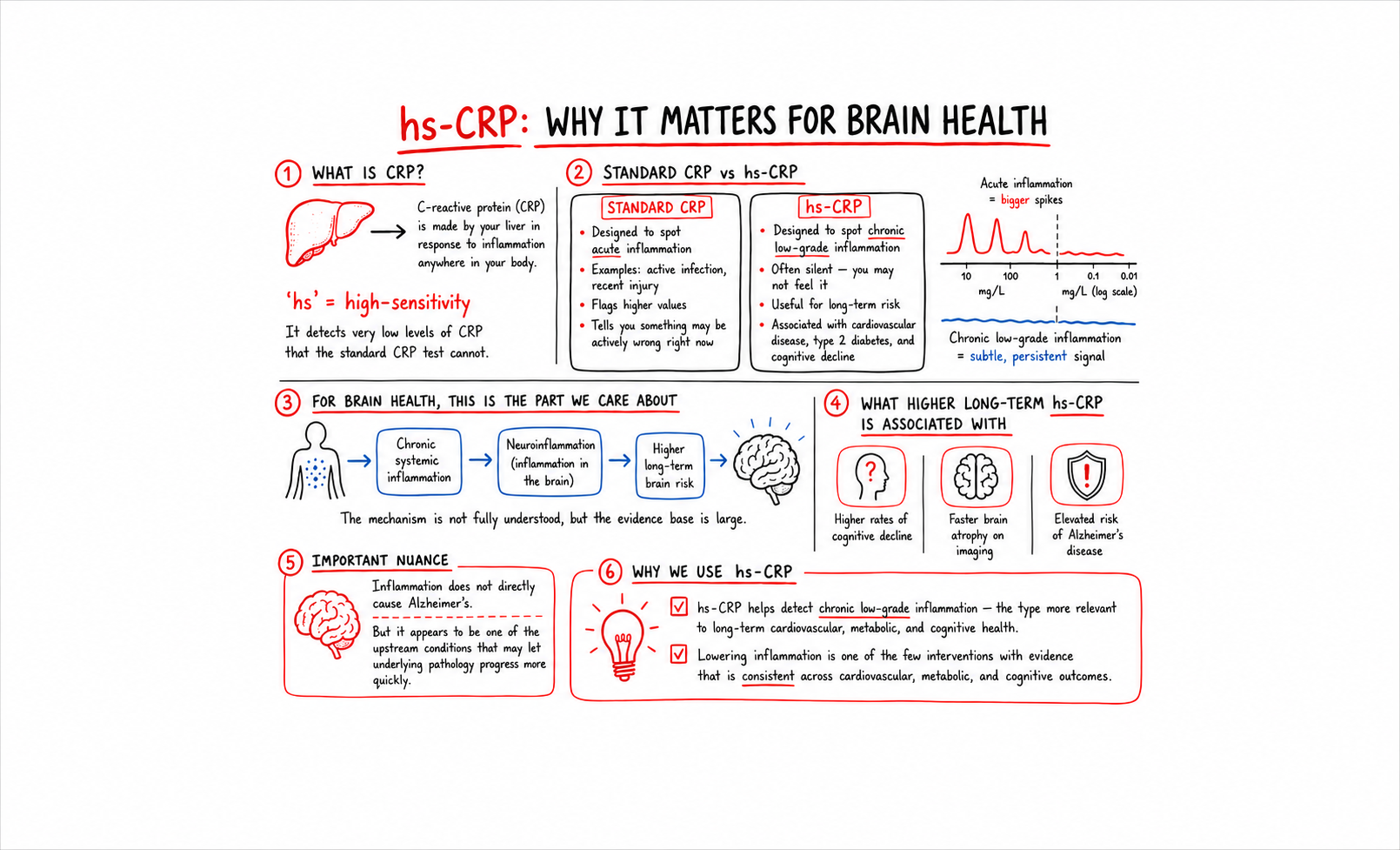
C-reactive protein is made by your liver in response to inflammation anywhere in your body. The "hs" stands for "high-sensitivity," which means the test can detect very low levels of CRP that the standard CRP test cannot.
This distinction sounds technical but it is the whole reason we use hs-CRP and not standard CRP. Standard CRP is designed to spot acute inflammation, like an active infection or a recent injury. The values it flags are high enough to indicate something is actively wrong right now. hs-CRP is designed to spot chronic low-grade inflammation, the kind that does not feel like anything but is associated with long-term risk for cardiovascular disease, type 2 diabetes, and cognitive decline.
For brain health, the chronic low-grade version is the one that matters.
Why this matters for your brain
Chronic systemic inflammation is associated with neuroinflammation, the inflammatory state of the brain itself. The mechanism is not fully understood, but the body of evidence is large. People with higher long-term hs-CRP have higher rates of cognitive decline, faster brain atrophy on imaging, and elevated risk of Alzheimer's disease.
Inflammation does not directly cause Alzheimer's. But it appears to be one of the upstream conditions that lets the underlying pathology progress more quickly. Lowering it is one of the few interventions where the evidence is consistent across cardiovascular, metabolic, and cognitive outcomes.
What the numbers mean
- Optimal: under 1.0 mg/L
- Borderline: 1.0 to 3.0 mg/L
- High: above 3.0 mg/L
Most standard labs flag a result only when it crosses 3.0 mg/L or higher. The 1.0 to 3.0 range is where a meaningful number of clients are quietly running elevated. Their primary care has waved it off as "in range." For brain health purposes, it is not.
The biomarkers that pair with hs-CRP
A single hs-CRP value is informative but more useful in context. The markers to look at alongside it:
Homocysteine. Elevated homocysteine is associated with both inflammation and methylation problems. If hs-CRP and homocysteine are both elevated, the inflammation is likely driven in part by nutrient gaps.
ApoB and Lp(a). Cardiovascular markers. Elevated hs-CRP plus elevated ApoB is a particularly bad combination for vascular brain health.
HbA1c and Fasting Insulin. Metabolic markers. Glycemic dysfunction drives systemic inflammation. If hs-CRP is elevated, look here next.
Ferritin. Iron storage. Elevated ferritin can indicate underlying inflammation, separate from iron status.
The picture you assemble from these markers tells you whether the inflammation is metabolic, vascular, nutrient-driven, or something else.
What to do about it
The interventions that consistently move hs-CRP overlap with the interventions that consistently move long-term cognitive trajectory. Sleep, glycemic control, omega-3 status, dental health, gut health, and visceral fat reduction are all associated with lower chronic inflammation over time. None of them are quick fixes. All of them compound.
For BetterBrain clients with elevated hs-CRP, the coaching protocol usually starts with the highest-leverage area their panel reveals. A client whose hs-CRP is elevated alongside high HbA1c starts with glycemic control. A client whose hs-CRP is elevated alongside high homocysteine starts with methylated B-complex and a closer look at folate, B12, and B6 intake. The technique is to follow the panel.
Find out where you stand
hs-CRP is one of the most useful brain-health markers in routine bloodwork, and one of the most commonly missed. If you have not had a high-sensitivity version of CRP measured in the past year, it is worth checking.
BetterBrain Blueprint covers hs-CRP alongside 50+ other markers and starts at $89 with insurance.
.png)
The Essential Techniques our coaches keep recommending for brain health
We use the term Essential Techniques inside BetterBrain a lot. Each BetterBrain Practice (Move, Sleep, Eat, De-Stress, and so on) is made up of specific techniques, and the Essential Techniques are the ones our panel of clinical advisors identified as the techniques with the greatest evidence and broadest applicability.
These are not techniques for a specific kind of client. They are the techniques worth considering for almost everyone thinking about long-term brain health, regardless of starting point, age, or risk profile. About 15 to 20 percent of the techniques in our library are Essential. The other 80 to 85 percent are context-dependent, applied when a client's panel or situation calls for them. A coach builds a personalized action plan by looking across the whole library, deciding which Essentials to elevate first and which context-dependent techniques to layer in. The Essentials are the foundation underneath every plan.
We asked some of our coaches what trends they are seeing across the clients they work with, and which Essential Techniques those trends keep pointing back to.
The post-meal walk (Move Practice)
Maggie works with clients across the metabolic-health side of our client base. The trend she keeps seeing: HbA1c and fasting insulin numbers creeping into pre-diabetic ranges, often without the client realizing it. Many of them are exercising, but most of them are not walking after meals.
"Ten minutes after each meal. That is the rule I get the highest compliance on, because nobody can argue they don't have ten minutes. And it does more than people expect."
This is one of the Essential Techniques in our Move Practice because the evidence is broad and the bar to entry is low. A short walk after eating blunts the post-meal glucose spike. Repeated over months, it is one of the most reliable ways we have seen to shift HbA1c, fasting insulin, and the metabolic conditions that drive midlife brain atrophy. The cost is nothing, the schedule disruption is minimal, and the long-term payoff compounds. It is essential because it works for almost everyone.
Consistent wake time and morning light (Sleep Practice)
Emily works with a large share of our clients who came to BetterBrain because of family history of dementia. The trend she keeps seeing: anxious clients arriving with long supplement lists, wanting to talk about pTau-217 and APOE4, while sleeping six or fewer hours a night.
"One night of four hours isn't really the question. The question is why someone is typically sleeping four or five hours at most. Patterns matter. What we identify from the first visit and where we end up is more than one night of poor sleep. Sleep is the foundation. Exercise goals, stress management, eating, they all land once sleep patterns are optimized."
The Essential Technique Emily points to first is in our Sleep Practice: a consistent wake time paired with morning light. The reason this is essential for almost everyone is the glymphatic system. Sleep is the period during which the brain runs its only clearance system, including the clearance of amyloid. A consistent wake time anchors the circadian rhythm, and morning light reinforces it. The evidence is strong, the intervention is free, and it works for clients in their 30s and their 70s.
Strength training (Move Practice)
Wendy works with many of our clients in their late fifties and sixties. The trend she keeps seeing: clients who are doing aerobic exercise faithfully, often three or four days a week, and skipping strength training entirely.
"I'm flexible with many aspects of a health plan, but strength training is one area I strongly encourage people not to overlook. The research connecting muscle mass and brain health after 50 is incredibly compelling, and maintaining strength now can have a major impact on long-term health and quality of life."
Strength training is another Essential Technique in our Move Practice. The reason it is essential, not optional: muscle is the primary site of glucose disposal in the body, the pathways linked to neurogenesis are responsive to resistance training, and sarcopenia is one of the strongest predictors of cognitive decline in older adults. The evidence supports two sessions a week, moderate intensity, sustained for at least six months. Bodyweight work and resistance bands are enough to start. The technique is essential because everyone past 30 is slowly losing muscle, and the cost of skipping it is too high.
Methylated B-complex (Supplement Practice)
Another trend we keep seeing across our client base: people arriving with homocysteine in the 11 to 14 range, told by their primary care that it is fine. The gap between what is flagged at most labs and what is optimal for brain health is one of the cleanest examples of where our framework differs from standard care.
The optimal range for homocysteine is under 9 μmol/L. Most labs flag a result only above 15. The 9 to 14 range is where a meaningful number of clients are quietly carrying elevated risk that has been waved off. A methylated B-complex moves the marker for the majority of clients within three months, and the cognitive payoff is real.
The Essential Technique in our Eat Practice is targeted methylated B-complex supplementation. The reason this is essential for almost everyone has to do with the underlying biology. Homocysteine is cleared through methylation pathways that depend on the active forms of folate, B12, and B6. A significant portion of the population carries variants of the MTHFR gene that reduce how well the body converts standard folic acid into the active form. Methylated B-complexes deliver the active forms directly. For anyone over 40 thinking about long-term brain health, this is one of the highest-leverage interventions available.
What the pattern reveals
Across our coaches with different specialties and different client populations, the same Essential Techniques keep coming up. These are the techniques that consistently move the needle, regardless of who is doing them. What our coaches actually do day to day is build action plans that span the full technique library, prioritizing among the Essentials and layering in the context-dependent techniques that fit each client's panel and life.
The Essentials are universal. The action plan is personal.
Find out where to start
If you'd like a quick read on which Essential Techniques to prioritize based on what you are already doing, take the free Essential Scan. Open to anyone, whether you're already a BetterBrain client or just starting.
If you'd like a deeper personalized action plan, BetterBrain coaching pairs you with a Brain Health Coach who builds the plan with you. Coaching is covered at $0 for 92% of approved clients with qualifying insurance.

Visceral Fat and the Brain: What 16 Years of Data Actually Show
A study just landed in Nature Communications that reframes how to think about midlife weight loss and brain health. Researchers followed 533 adults for up to 16 years after they completed lifestyle interventions, then scanned their brains and tested their cognition. The finding: it wasn't weight loss that predicted slower brain atrophy and better cognitive scores years later. It was sustained loss of visceral fat specifically.
This matters because most people, and most doctors, still track weight on a scale. The number on the scale lumps together fat, muscle, water, and where on the body the fat actually sits. The new data suggests that for brain health, where the fat is matters more than how much of it there is.
What the study found
The research, called the Follow-Interventions-Trials (FIT) project, pulled participants from four earlier 18 to 24 month lifestyle randomized trials. The average age at follow-up was 61. Each participant had abdominal MRI, brain MRI, and Montreal Cognitive Assessment (MoCA) testing 5 to 16 years after their original intervention.
Three findings stood out. Lower long-term visceral fat exposure, calculated across baseline, post-intervention, and follow-up, independently predicted higher cognitive scores. Visceral fat loss during the intervention period predicted higher brain volumes years later, independent of overall weight loss. And among the participants who had three full sets of scans over the years, lower long-term visceral fat was associated with a slower rate of brain atrophy.
The same patterns were not observed for subcutaneous fat, the kind that sits under the skin and shows up on a pinch test. Visceral fat, the deeper fat surrounding the organs, was the variable that mattered.
The proposed mechanism is glycemic. Visceral fat is metabolically active. It secretes inflammatory signals and contributes to insulin resistance. Both of these are increasingly understood as drivers of cognitive decline. When visceral fat goes down, glycemic control improves, and the brain appears to benefit downstream.
Why this changes how we think about midlife weight
Most people who decide to lose weight in their fifties do not distinguish between subcutaneous fat, visceral fat, and muscle. Many lose all three. Losing muscle in midlife is a problem on its own. Losing subcutaneous fat without losing visceral fat is largely cosmetic. Losing visceral fat appears to be the part that actually protects the brain.
This also reframes "skinny fat." A person can have a body mass index in the normal range and still carry significant visceral fat. The scale will not flag this. A waist measurement, a DEXA scan, or abdominal imaging will.
For anyone in their 40s, 50s, or 60s thinking about brain health, the practical question is no longer "should I lose weight." It is "what is my visceral fat doing, and what is actually moving it."
What you can do
Three things tend to move visceral fat without requiring dramatic restriction.
The first is reducing refined carbohydrates and added sugars. Visceral fat is more responsive to insulin signaling than subcutaneous fat. Lowering postprandial glucose spikes is associated with reduced visceral fat over time.
The second is consistent moderate-intensity movement, especially after meals. A 10 to 15 minute walk after eating blunts the post-meal glucose curve. Repeated over months, this contributes meaningfully to visceral fat reduction.
The third is strength training, which we covered last week. Muscle is the primary site of glucose disposal in the body. More muscle means better glycemic control, which means less visceral fat accumulation.
The biomarkers that respond, and the ones we look at first with members, are HbA1c (your average blood sugar over three months), fasting insulin, and the broader metabolic panel that looks at lipids and liver function. These shift before the scale shifts. They tell you whether the metabolic conditions that drive visceral fat are improving.
The bottom line
The next time someone tells you to lose weight for your brain, the more useful version of that advice is to lose visceral fat for your brain. The number on the scale was always a poor proxy for what is happening inside the body. The new research makes that clearer.
If you are already a BetterBrain member, your most recent HbA1c, fasting insulin, and metabolic panel results are in your dashboard. Worth a fresh look in light of this.
If you have not yet started, these markers are part of the BetterBrain Essentials Panel we look at first.
Get immediate insights with a 3 minute assessment
Start now.png)
GreyMatters
Grey Matters: June is Brain Awareness Month: a friendly reminder
A few reminders worth repeating
The fundamentals matter. Movement, sleep, nutrition, and social connection show up in the research again and again, and the earlier you start working on them, the more they compound.
But the fundamentals are just the starting point. Brain health is also deeply individual, and what moves the needle most for one person may not be what moves it for you. Depending on your biology, your genetics, your biomarkers, and your specific risk factors, the right plan might involve targeted supplementation, hormone or metabolic interventions, cardiovascular work, cognitive training, or addressing things like sleep apnea or inflammation. That's exactly why knowing your baseline matters so much. It turns a generic checklist into a plan built around you.
What our members are saying
"I put off getting tested for years because I figured there was nothing I could do. BetterBrain showed me exactly where I stood and gave me a plan. I wish I'd started sooner." — John O.
"Having a coach who actually checks in made all the difference. I've never been this consistent with my health." — Caroline T.
"Knowing my numbers took away the fear. Now it just feels like something I'm in control of." — Sandra W.
Consider this your friendly nudge
If brain health has been on your mind, this is a good month to act on it. Getting started is simple, much of it may be covered by insurance, and your future self will thank you.
And if you've already started on your BetterBrian journey consider forwarding this to a friend to help them take that next step.
Share this referral link and they'll get Essentials labs (50+ biomarkers) for just $39 (normally $89), plus access to $0 coaching with insurance.
Grey Matters: See the research behind every recommendation
Hey there,
There's a lot of brain health advice on the internet, and most of it comes with the same problem: no way to tell where it came from or if it's trustworthy. Someone tells you sauna is good for your brain, or that you should be lifting, or that omega-3s matter, and you're left to either take it on faith or go digging through PubMed yourself. Most people, reasonably, just take it on faith.
We've never loved that, because trust in health advice should be earned, not assumed. So we did two things worth telling you about.
The Content Library
First, if you haven't spent time in the Content Library inside your dashboard, it's worth a look. It's a growing, curated collection of the best brain health content we can find: videos, podcasts, articles, and clips, pulled from people who actually know what they're talking about. Think Andrew Huberman on light and sleep, Rhonda Patrick on sauna and exercise, our own CSO Tommy Wood on reducing cognitive decline, and a lot more.
You can search it, filter by format, and save what you want to come back to. And BeBe can point you to the right thing for wherever you are: if you ask about sleep, it can hand you the specific episode worth your time instead of making you wade through everything. It's the difference between a search engine and a good friend who's already done the reading. If you're not a BetterBrain client yet, you can access the Content Library for free with a Self-Directed account.
Technique Spotlight
The studies behind your plan
This is the part we're most excited about. Every technique and recommendation in your BetterBrain plan is now linked to the actual research behind it, the specific studies connected to the specific practice, biomarker, or system they support. When BeBe or your coach suggests something, you can trace it straight to the evidence and see how strong it is.
This was a big project and it brings roughly 1,500 studies into the app, mapped to the techniques and markers they relate to. Weak or unsupported studies were deliberately left out, so what's linked is the evidence we'd actually stand behind.
Here's why that matters. Not every recommendation carries the same weight. Some are backed by large randomized trials, others by smaller or observational work, and you deserve to know which is which. Linking the studies keeps us accountable to the evidence and lets you make informed decisions instead of just following instructions. It's the same standard we hold ourselves to internally: when a new study comes out, we read it, assess it, and only fold it into what we recommend if it holds up.
How this relates to brain health
Brain health is a field with real science and a lot of noise, and the two are easy to confuse. We try to stay on the science side of that line and be honest about what's solid, what's promising, and what's still an open question. Making the research visible is that principle made concrete. If we recommend it, you should be able to check it.
If you want to explore, open a technique and scroll to the bottom to see the relevant studies or ask BeBe why it recommends any technique in your plan, and follow the research yourself.
And if you're reading this as someone who hasn't started with us yet: this is what BetterBrain is, evidence-based brain health guidance you can verify, not wellness advice you have to trust blindly. BetterBrain coaching is covered at $0 for 92% of approved clients. See if you're covered.
Know someone who might benefit from BetterBrain?
Share this referral link and they'll get Essentials labs (50+ biomarkers) for just $39 (normally $89), plus access to $0 coaching with insurance.
An 11-country trial tested brain health advice against structured support
The same brain health advice produced very different results
Most people already know the broad advice for protecting their brain. Exercise regularly. Eat well. Manage blood pressure and blood sugar. Stay socially and mentally engaged. Get enough sleep.
The harder part is following through consistently, especially when work gets busy, routines change, motivation fades, or the original plan does not fit your life very well.
A two-year randomized trial across eleven Latin American countries has now put a number on how much that harder part is worth. Both groups worked on the same broad areas of brain health. One group received ongoing coaching, supervision, and regular group meetings. The other received health education and general recommendations. After two years, the structured group showed 55 percent greater improvement in overall memory, thinking, and reasoning.
The trial, called LatAm-FINGERS, was published in The Lancet and presented at the Alzheimer's Association International Conference.
What the trial tested
The study included 1,065 older adults who were at elevated risk of cognitive decline but did not have dementia. It ran across twelve sites in eleven countries and followed participants for two years.
Both groups worked on the same broad areas of brain health, including physical activity, nutrition, cognitive training, social engagement, and management of cardiovascular risk. The difference was the amount of structure surrounding the work.
The flexible group, 526 participants, attended four meetings over two years. They received health education and general recommendations, but no ongoing coaching or supervision.
The structured group, 539 participants, received supervised exercise, nutrition counseling, cognitive training, cardiovascular risk monitoring, ongoing coaching, and 38 group meetings that provided social connection and accountability.
In other words, the trial was not testing whether lifestyle matters for the brain. That question has been asked before. It was testing how much the way a program is delivered can change the results it produces.
What happened
After two years, the structured group showed 55 percent greater improvement in overall memory, thinking, and reasoning than the more flexible group. They also had greater improvements in executive function and processing speed.
Both groups were working on their brain health, and both improved. The structured group simply improved much more.
That makes the finding more interesting than a comparison between doing something and doing nothing. The broad recommendations were similar. What changed was the frequency of contact, the level of supervision, and the support participants received while putting those recommendations into practice.
Because participants were randomly assigned to the two groups, differences in motivation or baseline health are less likely to explain the result. The structured program itself appears to have contributed to the additional cognitive improvement.
Heather Snyder of the Alzheimer's Association, commenting on the results at the conference, put it simply: "A key message from this study is that structure and social support matter."
The finding builds on the original FINGER trial in Finland, which found that a multidomain lifestyle program could help protect cognitive function in older adults at risk of decline. LatAm-FINGERS took that model and adapted it to local cultures, diets, and habits rather than importing it unchanged, which matters for anyone wondering whether these programs travel.
Read the full LatAm-FINGERS study
What structured support actually does
A brain health plan can look simple on paper and still be difficult to carry out.
A person may leave an appointment intending to exercise four times a week, improve their sleep, change their diet, take several supplements, and reduce stress. Every recommendation may be reasonable. The problem is that seven reasonable priorities are still seven priorities competing with the rest of life.
A few weeks later, the easiest habits are sometimes still happening. The more inconvenient ones have started to disappear, which is where structured support comes into play. It creates a regular opportunity to review what happened, understand why something did not work, and adjust the action plan before one missed week becomes a habit that has quietly been abandoned.
Sometimes the person needs accountability. Sometimes the goal was too ambitious. Sometimes the recommendation needs to change because of travel, an injury, family responsibilities, or a demanding period at work.
The goal is not to follow the original plan perfectly. It is to keep adjusting the plan until it works in real life.
The question the study leaves open
LatAm-FINGERS compared a structured, intensive program with a more flexible, self-guided version focused on the same broad areas of brain health. It did not test whether a personalized action plan works better than a generic one. That is a separate question, and an important one.
Two people can receive the same list of brain health recommendations and have very different needs. One person may need to focus on blood pressure. Another may need to address poor sleep, low cardiovascular fitness, insulin resistance, or a nutritional deficiency first. The markers that shape brain health sit across sleep, metabolic health, cardiovascular health, inflammation, and nutrition, and they do not line up the same way in any two people.
A useful brain health system needs to answer two questions. What matters most for this person, and what will help them keep doing it?
Personalization helps determine the priorities. Structure helps turn those priorities into sustained action.
How BetterBrain approaches both
BetterBrain is one connected system that brings together brain-relevant health information, a personalized action plan, and continued support.
There are two ways to start.
Some people begin with Blueprint, which uses more than 50 brain-relevant biomarkers, cognitive testing, health history, and lifestyle information to identify the areas that matter most for their brain health, with a nurse coach to walk through what the results mean. Instead of receiving a broad list of everything they could improve, they get a personalized action plan ranked by impact.
Others begin with the Coaching Program, where a dedicated brain health coach helps build the action plan, checks in on progress, and adjusts it when life gets in the way. Coaching is often fully covered by insurance, and many commercially insured clients pay nothing out of pocket.
Both starting points lead toward the same goal: a smaller set of meaningful priorities, a realistic action plan, and enough continued support for that plan to last.
The bottom line
The LatAm-FINGERS trial moves the brain health conversation beyond whether lifestyle matters. It shows that the way lifestyle guidance is delivered can meaningfully change the outcome.
Advice alone leaves people responsible for setting priorities, creating a schedule, tracking progress, solving barriers, and knowing when to adjust the plan. A better delivery system does those things with them. It provides clear priorities, regular contact, accountability, opportunities to review progress, and a way to adapt when the original plan stops working. That support helps healthy actions continue long enough to produce meaningful results.
Personalization helps you choose the right actions. Structure helps you keep doing them.
How to Keep Your Brain Sharp at Any Age: 6 Lessons From Dr. Tommy Wood on Huberman Lab
Our Chief Science Officer, Dr. Tommy Wood, joined Andrew Huberman on the Huberman Lab podcast for a nearly three-hour conversation titled "Accelerate Learning & Increase Cognitive Capacity." His core message: your brain keeps adapting to whatever you ask of it, at 40 and at 75. Staying sharp is less about your age and more about whether you keep giving your brain new, challenging inputs, move your body before and around mental work, eat a high-quality overall diet, and test your biomarkers instead of guessing at supplements.
Here are the six takeaways we think are most worth acting on, plus where to start if you want to put them into practice.
Does aging itself cause cognitive decline?
Not in the way most people assume. According to Wood, aging itself is not the primary driver of decline. Your brain keeps the capacities you use and prunes the ones you stop using, so much of what we call age-related decline comes from no longer giving the brain new, challenging inputs. Encouragingly, he notes that mental processing speed tends to hold steady until around age 60.
That reframing matters. If decline is largely about disuse rather than age, then the inputs you choose, at any age, are levers you control.
What activities actually keep your brain sharp?
The activities that build cognitive capacity share three traits: they are new, hard, and ideally social.
Crosswords and sudoku, Wood points out, are more relaxing than challenging. They exercise skills you already have. To actually build capacity, pick something that stretches you and mixes movement, thinking, and other people:
- Dancing has the best evidence, ballroom and square dancing especially
- Ball sports and martial arts
- Learning a language
Part of the trick is getting comfortable being a beginner. The discomfort of making mistakes is not a sign you picked the wrong activity. It is what drives the learning.
Do you need to be in a flow state to learn?
No. Real learning, and even peak performance, often happens in what athletes call a clutch state, where the work still feels like hard work.
What matters more is structure. Hard mental work is really only sustainable in 20 to 30 minute focused blocks, so work in chunks and protect them from distraction. Even having a phone in the room carries a cost to focus.
How does exercise improve learning and memory?
Wood describes exercise as two brain tools in one:
- In the moment: a short 20 to 30 minute jog or strength session right before mental work sharpens learning during that session.
- Over time: harder aerobic work, like intervals, builds the hippocampus and supports memory, while resistance training builds the brain's white matter and supports decision-making.
The practical answer to "cardio or weights for brain health?" is both, and if you can, schedule some of it right before your most demanding mental work.
What should you eat, and should you take supplements?
On diet, whole-food patterns like the Mediterranean and MIND diets have the best evidence, and it is overall diet quality, not any single food, that matters.
On supplements, Wood's advice is to test your levels rather than guess, because the standard "normal" lab range is not the same as the optimal one. His clearest example: omega-3 and B vitamins only work when you have both. That interdependence is exactly why we measure homocysteine and other brain-specific biomarkers in Blueprint rather than blanket-recommending a supplement stack.
For supplements with modest, real support, he points to creatine and a basic omega-3 plus B-vitamin stack. Our picks in those categories, including Advanced DHA, Thorne Creatine, and MethylAssist, are all in the Picks library, and Picks is now HSA/FSA eligible through our partnership with TrueMed.
What else protects long-term brain health?
Some of the biggest protections are indirect. Blood pressure, cholesterol, hearing, and metabolic health all shape long-term brain health. Avoiding serious illness matters too, because cognition tends to step down after a major sickness rather than declining smoothly.
One finding Wood flags as worth watching: the shingles vaccine has been associated with lower dementia risk across several large studies.
Where to start
You do not need a perfect routine or new technology. The conversation points to a short list: work on something hard and a little new, move before mental work, get real sleep, and test before you supplement.
That last step is where BetterBrain can help. Blueprint covers the testing, 50+ biomarkers plus cognitive testing and a 1:1 consultation to walk through your results, for $89 with insurance. And if you finish your results thinking "okay, but what should I actually do," that is what our 12-week Coaching Program is for. 92% of eligible customers pay $0 with insurance.
If you want to go deeper, listen to the full episode, and check out Tommy's new book, The Stimulated Mind: Future-Proof Your Brain from Dementia and Stay Sharp at Any Age, which covers the same ground in more depth through his 3-S model: challenge the brain, feed it, and let it recover.
Frequently asked questions
At what age does cognitive decline start?
Later than most people think. Wood notes that mental processing speed tends to hold steady until around age 60, and that much of what we attribute to aging actually reflects reduced challenge. The brain keeps what you use and prunes what you stop using, at any age.
Are crosswords and sudoku enough to keep your brain sharp?
Probably not. Wood describes them as more relaxing than challenging, since they exercise skills you already have. To build new capacity, choose activities that are new, hard, and social, like dancing, ball sports, martial arts, or learning a language.
What is the best exercise for brain health?
Both aerobic and resistance training, for different reasons. Harder aerobic work like intervals builds the hippocampus and supports memory, while resistance training builds white matter and supports decision-making. A 20 to 30 minute session right before mental work also sharpens learning in the moment.
Should I take supplements for brain health?
Test first. Standard "normal" lab ranges are not the same as optimal ranges, and some nutrients depend on each other. Omega-3 and B vitamins, for example, only work when you have both, which is why measuring biomarkers like homocysteine beats guessing. Creatine and a basic omega-3 plus B-vitamin stack have modest, real evidence behind them.
You Can Now See the Studies Behind Every BetterBrain Recommendation
There's a lot of brain health advice on the internet, and most of it comes with the same problem: no way to tell where it came from or whether it's trustworthy.
Someone tells you sauna is good for your brain. Or that you should be lifting. Or that omega-3s matter. And you're left to either take it on faith or go digging through PubMed yourself. Most people, reasonably, just take it on faith.
We've never loved that. Trust in health advice should be earned, not assumed. So we did two things worth telling you about.
The Content Library: curated, not crowdsourced
If you haven't spent time in the Content Library inside your dashboard, it's worth a look. It's a growing, curated collection of the best brain health content we can find: videos, podcasts, articles, and clips from people who actually know what they're talking about.
Think Andrew Huberman on light and sleep. Rhonda Patrick on sauna and exercise. Our own Chief Science Officer, Dr. Tommy Wood, on reducing cognitive decline. And a lot more.
You can search it, filter by format, and save what you want to come back to. And BeBe, our AI assistant, can point you to the right thing for wherever you are. Ask about sleep, and it hands you the specific episode worth your time instead of making you wade through everything. It's the difference between a search engine and a good friend who's already done the reading.
Not a BetterBrain client yet? You can access the Content Library for free with a Self-Directed account.
The studies behind your plan
This is the part we're most excited about.
Every technique and recommendation in your BetterBrain plan is now linked to the actual research behind it: the specific studies connected to the specific practice, biomarker, or body system they support. When BeBe or your coach suggests something, you can trace it straight to the evidence and see how strong it is.
This was a big project. It brings roughly 1,500 studies into the app, each mapped to the techniques and markers it relates to. Weak or unsupported studies were deliberately left out, so what's linked is the evidence we'd actually stand behind.
Why evidence strength matters
Not every recommendation carries the same weight. Some are backed by large randomized controlled trials. Others rest on smaller or observational work. You deserve to know which is which.
Linking the studies does two things. It keeps us accountable to the evidence. And it lets you make informed decisions instead of just following instructions.
It's the same standard we hold ourselves to internally: when a new study comes out, we read it, assess it, and only fold it into what we recommend if it holds up.
Why this fits how we think about brain health
Brain health is a field with real science and a lot of noise, and the two are easy to confuse. We try to stay on the science side of that line and be honest about what's solid, what's promising, and what's still an open question.
Making the research visible is that principle made concrete. If we recommend it, you should be able to check it.
How to explore
Open any technique in your plan and scroll to the bottom to see the relevant studies. Or ask BeBe why it recommends any technique in your plan, and follow the research yourself.
And if you're reading this as someone who hasn't started with us yet: this is what BetterBrain is. Evidence-based guidance to sharpen your brain health now and reduce dementia risk long-term, backed by research you can verify rather than wellness advice you have to trust blindly. BetterBrain coaching is covered at $0 for 92% of approved clients. See if you're covered.
Bottom line
The Content Library puts the best brain health content in one curated place. And every technique in your plan is now linked to the real research behind it.
Trust in health advice should be earned. Now you can check ours.
How Chronic Stress Shrinks Your Brain, and How to Reverse It
Chronic stress does more than affect your mood. Sustained cortisol exposure physically shrinks the hippocampus, your brain's primary memory center. The encouraging part: this is reversible. In controlled neuroimaging studies, eight weeks of mindfulness practice increased gray matter in the hippocampus and reduced it in the amygdala, the brain's threat-detection center. Managing stress is one of the most accessible ways to protect your long-term cognitive health.
Stress is easy to file under "quality of life" rather than "brain health." The neuroscience tells a different story, and it's a hopeful one, because the same biology that makes chronic stress harmful also makes it one of the most modifiable risks you can act on.
Below, we cover what chronic stress does to the brain, the landmark study showing mindfulness can reverse it, the techniques that actually work, and how to measure your progress.
What does chronic stress do to your brain?
When your brain perceives a threat, it releases cortisol. In short bursts, this is helpful, it sharpens your response to a genuine challenge. The problem is sustained elevation.
Under chronic stress, prolonged cortisol exposure becomes toxic to neurons, and the hippocampus is especially vulnerable because it is packed with cortisol receptors. Over time, that exposure causes the neural branches that let brain cells communicate to shrink. The downstream effects are measurable: reduced hippocampal volume, fewer new brain cells, and impaired memory.
This matters beyond day-to-day forgetfulness. Hippocampal shrinkage is one of the earliest detectable structural changes in Alzheimer's progression, and chronic psychological stress is now recognized as a modifiable dementia risk factor in its own right. In other words, stress sits on the same biological pathway as accelerated cognitive aging, which is precisely why acting on it has such a high return.
Can mindfulness reverse stress-related brain changes?
Yes, and the evidence comes from before-and-after brain imaging, not self-report.
In 2011, researchers at Harvard-affiliated Massachusetts General Hospital published a landmark neuroimaging study. Using MRI, they measured gray matter density in healthy adults before and after eight weeks of mindfulness practice. Participants showed measurable increases in gray matter in the hippocampus and in regions involved in learning and emotional regulation. At the same time, gray matter in the amygdala, the brain's primary stress and threat-detection center, decreased. A control group who did not practice mindfulness showed none of these changes.
The design is what makes it compelling. This was not a comparison of lifelong meditators against non-meditators, where genetics or lifestyle could explain the difference. It was imaging of the same brains, across just eight weeks of practice. You can read the full study here.
How does stress management protect the brain?
Mindfulness and related practices work through a few overlapping mechanisms. They reduce cortisol output, calm the amygdala's threat response, and lower the chronic, low-grade inflammation associated with sustained stress. These are the same pathways implicated in accelerated cognitive aging, so quieting them protects the brain on more than one front at once.
The practical implication is freeing: you do not need the "perfect" technique. You need to move these levers consistently, and there is more than one way to do that.
What stress management techniques actually work?
Different techniques reach the same biology through different doors, which means you have options. These are the Essential, evidence-based interventions to start with:
- Slow, deep breathing. Controlled breathing activates your parasympathetic nervous system, your body's "rest and digest" mode. Even a few minutes measurably reduces cortisol and heart rate. For many people this is the easiest entry point.
- Mindfulness meditation. The technique behind the brain-imaging study above. Consistent practice, even 8 to 10 minutes daily, produces measurable effects on stress hormones and self-reported stress within a few weeks.
- Nature exposure. Time in natural environments is associated with lower cortisol, lower blood pressure, and improved mood. The effect appears to be dose-dependent, so more time outdoors tends to help more.
- Social support. Strong social connections help buffer the brain against the effects of stress.
How do you start a 10-minute mindfulness practice?
You do not need a cushion, an app, or a quiet mind. Here is the whole practice:
Find a quiet spot and sit comfortably. Bring your attention to the physical sensation of your breath, the air moving in and out. Your mind will wander. That is not failure, that is the exercise. Each time you notice it drifting and bring it back, you are doing the rep that builds the skill. There is no perfect posture and no requirement to empty your mind. Just ten minutes of practicing the return.
A note on getting started: Don't overthink which technique to begin with. If sitting meditation feels like a stretch, start with a few minutes of slow breathing or a walk outside. The research is clear on this point: the technique that protects your brain is the one you will actually do.
How can you track stress and its effects on the brain?
You can't feel your inflammation dropping, but you can measure it. Chronic stress shows up in bloodwork as elevated hs-CRP, one of the same inflammatory markers associated with cognitive decline. When a stress-management practice starts working, that number moves, and lab panels let you watch it happen.
The effects ripple outward from there. Sleep quality typically improves within weeks of consistent practice, and better sleep gives your glymphatic system, your brain's overnight waste-clearance crew, more time to do its job.
This is what makes stress management such a high-leverage intervention. It rarely works alone. Better stress regulation improves your sleep, better sleep amplifies the benefits of exercise, and lower inflammation makes anti-inflammatory nutrition work harder. Pull one lever, and the whole system responds.
The bottom line
Chronic stress physically changes the structure of your brain, and mindfulness and related practices can measurably change it back. You don't need to overhaul your life to benefit. Ten minutes of breathing or meditation, a walk outside, or time with people you care about all move the same biology. Start with whatever feels easiest, stay consistent, and let the results compound.
If you're working with a Brain Health Coach, the De-Stress section of your protocol is a natural starting point.
Ready to build a personalized stress management practice? Check if your insurance covers coaching.
Frequently asked questions
Does stress really shrink your brain?Yes. Sustained cortisol exposure from chronic stress is associated with reduced hippocampal volume, the brain region responsible for memory. It also reduces the formation of new brain cells and impairs memory over time.
Can you reverse brain changes caused by stress?Evidence suggests you can. In a 2011 MRI study, eight weeks of mindfulness practice increased gray matter in the hippocampus and decreased it in the amygdala in the same participants, changes not seen in a non-practicing control group.
How long does it take for mindfulness to change the brain?Structural changes were measurable after eight weeks of practice in controlled imaging studies, and effects on stress hormones and self-reported stress often appear within a few weeks.
What is the best stress management technique for brain health?There is no single best technique. Slow breathing, mindfulness meditation, nature exposure, and strong social connection all work through overlapping pathways. The most effective one is the one you will do consistently.
Is chronic stress a risk factor for dementia?Chronic psychological stress is now recognized as a modifiable dementia risk factor. Hippocampal shrinkage, which stress contributes to, is one of the earliest structural changes seen in Alzheimer's progression.